Watery Diarrhea & Frequent Fecal Dribbling in a Cat
Elin Maki, MS, DVM candidate, Kansas State University
Lisa M. Pohlman, DVM, MS, DACVP, Kansas State University
History
An approximately one-year-old, intact female domestic medium-hair cat was relinquished to a humane society. The cat had been owned for a month after being found as a stray. The cat was very friendly, which suggested it had previously been handled by humans. The cause of surrender was reportedly chronic diarrhea of at least a month’s duration, with frequent dribbling of fecal matter that did not resolve with a 5-day course of fenbendazole (50 mg/kg PO every 24 hours).
On intake to the humane society, the cat tested negative for both FIV and FeLV, was vaccinated against rabies and FVRCP, and received nitenpyram (11.4 mg PO) and topical selamectin (45 mg). A sample of diarrheic feces was submitted for fecal flotation and assessment for Giardia spp antigen; no parasites or ova were found on fecal flotation and no Giardia spp antigen was detected. On physical examination the following day, the cat was bright, alert, and responsive, with normal vital signs. She was thin (5.9 lb [2.7 kg]) with a BCS of 3/9. During the examination, a small amount of clear, very slightly brown-tinged watery diarrhea dribbled from the patient’s anus. A wet mount and smear of the fluid were immediately prepared.
Diagnosis
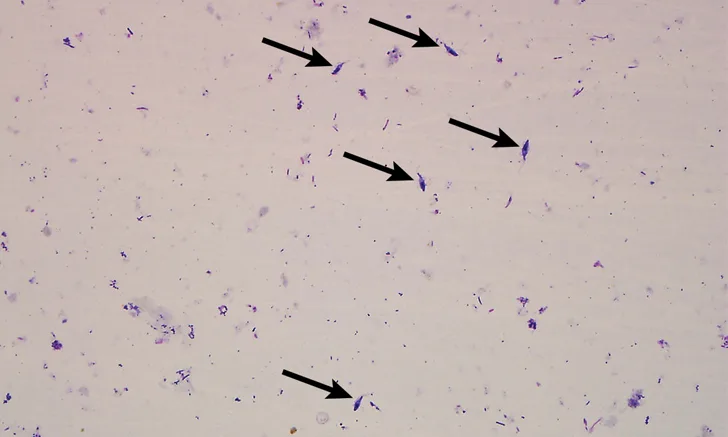
The wet mount revealed abundant motile organisms exhibiting rapid, forward progressive movement. The air-dried smear (Figures 1 and 2) revealed a variety of bacteria (mostly rods), debris, and protozoal organisms (9-12 µm x 6-9 µm) with 3 anterior flagella, one posterior flagellum, one nucleus, and an undulating membrane. Based on morphology, a presumptive diagnosis of Tritrichomonas foetus was made and subsequently confirmed via culture using an additional fresh fecal sample collected directly from the rectum.

Air-dried smear of watery, clear fluid that dribbled from the cat’s anus. A variety of bacteria (mostly rods), debris, and protozoal organisms (arrows) can be seen. Modified Wright’s stain, 400x magnification

Air-dried smear of watery, clear fluid that dribbled from the cat’s anus showing trichomonads ≈9 to 12 µm in length, 3 anterior flagella (asterisks), one posterior flagellum (curved arrows), one nucleus (straight solid arrow), and an undulating membrane (dashed arrows). Together, these features are consistent with T foetus infection. A variety of bacteria (mostly rods) and amorphous debris are also visible. Modified Wright’s stain, 1000x magnification
Treatment & Long-Term Management
The patient was prescribed ronidazole (30 mg/kg PO once daily for 14 days) and a high-protein diet (to address the malnutrition) and was isolated from other cats. The cage was thoroughly cleaned daily with soap and water, followed by a 0.5% accelerated hydrogen peroxide disinfectant. Disposable cardboard litter boxes were used and changed at least once daily (more if fecal material was identified in the box). Bedding was changed daily. Diarrhea slowly improved. Stools were soft but formed by the end of ronidazole therapy and normal by 14-days post-treatment. Follow-up culture submitted 2 weeks after completion of ronidazole treatment was negative.
The patient was spayed and adopted to a home as the only cat. At the 6-month follow-up, she had gained weight (7.9 lb [3.6 kg]), and the owner reported that she was energetic and had no further episodes of diarrhea.
TREATMENT AT A GLANCE
The treatment of choice for T foetus infection is extra-label use of ronidazole (30 mg/kg PO every 24 hours for 14 days). Treatment may need to be repeated, but the dose should not exceed 30 mg/kg.10-12
Resolution of clinical signs may not indicate absence of infection.
Patients that test positive for T foetus should be isolated while they are being treated, and litter boxes and food/water dishes should be disinfected frequently.9
Discussion
T foetus is a pathogenic trichomonad that causes chronic large-bowel diarrhea in young cats. A small percentage of cats with T foetus infection may display weight loss and signs of depression in addition to diarrhea.1 This species of pathogenic trichomonad also causes reproductive disease in cattle, although there are genetic2 and pathologic3 differences between cattle and cat isolates, suggesting interspecies transmission may not be of pathologic concern.4
Detection of T foetus infection in cats can be performed via fecal culture, PCR, wet-mount microscopic evaluation of fresh feces, or cytology of a stained fecal smear. However, the latter 2 options commonly result in false-negative results.4 Differential diagnoses for motile trophozoites on a fecal wet mount include T foetus, Pentatrichomonas hominis, and Giardia spp infection.4 Because trichomonads and Giardia spp are of similar size, confusion between them is common. Trichomonads can be identified by their rapid, forward progressive motility—a motion not exhibited by Giardia spp.4 Morphologic differentiation between trichomonads and Giardia spp can be performed via light microscopy of a stained fecal smear. If the organism’s structure is well-preserved—which allows anterior flagella to be counted easily— differentiation of P hominis and T foetus may also be performed via light microscopy of a stained smear. P hominis exhibits 5 anterior flagella, whereas T foetus exhibits 3 anterior flagella.5 The significance of differentiating the trichomonads is that P hominis is generally believed to be a nonpathogenic commensal parasite of the mammalian intestinal tract. However, a recent report suggests that P hominis should be considered an etiologic agent for feline chronic diarrhea in immunosuppressed cats.6
T foetus spreads in multiple-cat environments via the fecal–oral route.4 It is potentially transmitted via water, urine, dry and canned cat food, and feces.7 T foetus can survive for as long as 24 hours in a moist environment at room temperature.4,8
Resolving a T foetus infection can be challenging, especially in multiple-cat households. Cats that clear the initial infection are not immune to reinfection.4 Ideally, if one cat is positive, all cats in the home should be tested to prevent reinfection from a subclinical carrier. However, although a positive test result indicates infection with T foetus, a negative test result does not rule out infection. Animals that test positive for T foetus should be isolated while they are being treated, and litter boxes and food/water dishes should be disinfected frequently.9
Extra-label use of ronidazole (30 mg/kg PO every 24 hours for 14 days) is the treatment of choice for T foetus infection.10-12 Ronidazole at doses >30 mg/kg can cause neurologic signs, vomiting, and decreased appetite, and ronidazole should not be used in lactating queens or very young kittens.4 Patients may not improve after one course of treatment or may relapse after resolution of clinical signs.1 If clinical signs recur, the patient should be retested and, if positive, treatment can be repeated; however, a dose >30 mg/kg should not be used.4 Some T foetus strains are resistant to ronidazole, and repeated treatment may fail.9 Other potential causes of treatment failure include poor stability of ronidazole (it must be obtained from a compounding pharmacy) and inappropriate storage of the drug (medication must be kept in the freezer).10
Resolution of clinical signs does not guarantee absence of infection.10 For treated cats that test negative for the organism, it is uncertain whether ronidazole has actually cleared the infection or only suppresses the infection to a concentration lower than the detection limit.13 Although negative test results do not absolutely rule out infection, negative test results that are obtained on several different occasions build the strongest case for the absence of T foetus infection.9 Clinical signs may spontaneously resolve without treatment within 2 years, but chronic infections, with carrier status beyond resolution of clinical signs, are common and apparently resolved cats may develop diarrhea from T foetus years later.14
TAKE-HOME MESSAGES
T foetus infection should be considered in young cats with chronic large-bowel diarrhea, especially those in multiple-cat environments.4,10
Detection of rapid forward progressive motile trophozoites on a wet mount can provide a presumptive diagnosis of trichomonad infection, but false-negative results are common.4,9,10
PCR and culture are the most reliable methods of T foetus infection detection in cats.4,10
T foetus is transmitted via the fecal–oral route.4,10
T foetus can survive up to 24 hours in a moist environment at room temperature.4,8