Treatment of Ectopic Ureters
Daniel Degner, DVM, Diplomate ACVS, Michigan Veterinary Specialists, Auburn Hills, Michigan
The most common cause of urinary incontinence in juvenile intact female dogs is ectopic ureter (EU). This condition results from an aberration in embryologic development in which the terminal ureteral opening is located at a site other than the bladder trigone.
Urinary incontinence in these cases may be attributable to the positioning of the ureteral opening distal to the urethral sphincter and/or a poorly developed proximal urethra sphincter with disruption of the smooth muscle layer of the proximal sphincter. An EU usually enters the bladder wall at the level of the trigone, passes distally within the wall of the urethra, and then opens in the urethra distal to the urethral sphincter.The EU may also terminate in the vagina, cervix, or uterus, but that anomaly is much less common.
Diagnosis of Ectopic Ureter
Clinical Signs
Continuous and intermittent urinary incontinence are the major signs in very young female dogs.
Contrast Radiography
A normal terminal ureter has a “J” shape as it enters the bladder, whereas an EU will frequently course straight caudally beyond the bladder (Figure 1, arrow). This indicator provides the correct diagnosis in about three quarters of cases.
Ultrasonography
While performing the ultrasound, look for a dilated ureter alongside the neck of the bladder and urethra. The absence of ureteral jetting (urine expelled from the ureters into the bladder) may be a sign of an EU.
Contrast-Enhanced Computed Tomography (CT)
This is the best diagnostic imaging modality for the diagnosis of EU (Figure 2). Shown are the dilated EU (large arrow) and nondilated EU (smaller arrow), both within the urethral wall.
Urinary Endoscopy
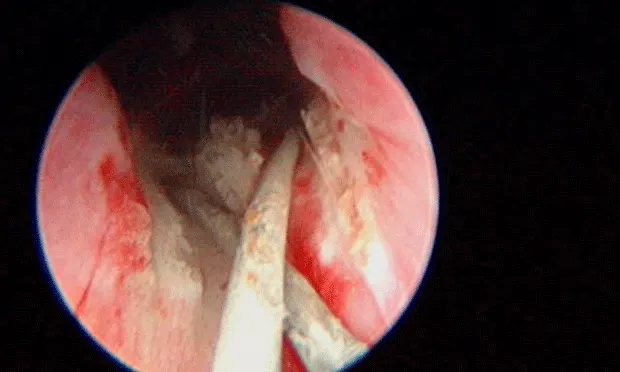
An experienced endoscopist can usually identify EUs (Figure 3, arrows; U = urethra lumen).



(Photo courtesy of Dr. John Kruger, Michigan State University)
Step-by-Step: Treatment of Ectopic Ureters
Resective & Ligation Neoureterostomies: Neoureterostomy is the most common open surgical technique performed in dogs and cats with an ectopic ureter. There are 2 modifications of this technique—resective and ligation.
Resective Neoureterostomy
Step 1
A ventral midline celiotomy that extends from the pubic bone to the cranial one third of the abdomen is performed. The ureters are examined as they pass caudally in the retroperitoneal space to the bladder. In most patients, the EU enters the bladder at the level of the trigone; thus on the external examination, the ureters and bladder may appear normal. About 50% of patients, however, will have hydroureter, which is obvious at time of surgery.
Author Insight
Counseling the client before surgery is critical, as the patient may not become continent after surgery if the urinary sphincter is poorly developed.
Step 2
A ventral cystotomy and cranial urethrotomy are performed. Stay sutures are placed along the sides of the bladder and urethra. The trigone is examined for the presence of a normal ureteral opening. Frequently the EU can be seen as a tubular bulge through the submucosa of the bladder and urethra.

Step 3
The opening of the EU is catheterized to help identify the structure during the dissection. A mucosal incision is made on the lateral side of the EU and the ureter is then dissected from the submucosal tissue using a pair of fine Metzenbaum scissors, taking care to preserve the underlying smooth muscle.

Step 4
The ureter is liberated from its bed to the level of the trigone of the bladder. The ureter is transected obliquely leaving a 3- to 5-mm stump and then spatulated by making a longitudinal incision in the dorsal bladder mucosa and ventral ureteral wall.

Step 5
An interrupted or continuous suture pattern is used to appose the mucosa of the ureter to the mucosa of the bladder. The length of the dorsal intraluminal urethral and bladder mucosal incision is then c losed in a continuous pattern with 5-0 pol yglactin 910. The thin layer of musc le should be incorporated in the closure, which results in a urethroplasty.

Step 6
The ventral urethrocystotomy incision is closed in a simple continuous pattern using 4-0 Monocryl (ethicon.com).

Ligation Neoureterosomy
The ligation neoureterostomy can be used only if the EU runs intraluminally in the area of the trigone. If the ureter runs outside the bladder wall and then joins the urethra or vagina, the ureter requires surgical reimplantation into the bladder.
Ligation neoureterostomy is a simpler technique than the resective; however, it may have theoretical disadvantages including recanalization, inability to surgically tighten the area of the proximal urethral sphincter mechanism, and urine stasis in the blind end of the distal EU, which may result in recurrent urinary tract infection.
One study showed similar clinical outcomes when comparing the resective versus ligation neoureterostomy techniques. This study did not discuss whether urethroplasty (tightening) was concurrently performed with the resective technique. The primary challenge of the ligation neoureterostomy technique is identification of the ureters within the wall of the trigone.
Improper identification of the EUs may result in failure to capture the ureters within the encircling ligature. Applying digital compressive pressure to the EUs distal to the trigone may dilate them with urine for easier identification.
Author Insight
Catheterization of the EU can help identify the abnormal structure and simplify the surgery.
Step 1
The ligation neoureterostomy is performed via ventral cystostomy incision. A longitudinal incision is made into the ectopic intramural ureter in the trigone region of the bladder.

Step 2
The ureter is catheterized just distal to the neoureterostomy and a linear incision is made through the bladder mucosa, but not through the ureter. A ligature of polydioxanone or polypropylene is placed around the ureter just distal to the neoureterostomy site and is tied as the catheter is withdrawn.

Step 3
The bladder mucosal incision is apposed with fine suture to the incised urethral mucosa at the neoureterotomy site. As an alternative, the suture may be placed and tied around the EU from the outside of the bladder. The ventral cystotomy incision is closed routinely.

Cystoscopic-Assisted Laser Surgery
In one study, 4 of 13 patients had complete resolution of urinary incontinence with laser surgery alone, 5 of 13 had complete resolution with laser surgery and phenylpropanolamine and 4 of 13 remained incontinent.
It is important to note that this procedure can be used only for intramurally located EUs.
Step 1
By way of urethroscopy, the EU is catheterized with a polypropylene catheter or guide wire.

Step 2
A diode laser or radiofrequency is used to longitudinally incise the ureter from the ectopic ureteral orifice to the level of the trigone.

A
The plastic stent has been placed in the EU and the laser (green tip) is ablating the tissue over the stent.
Author Insight
If the patient fails to respond to surgery alone, the addition of phenylpropanolamine may improve urinary continence.
Postoperative Care
Indwelling urinary catheter: An indwelling urinary catheter should be placed if urethral swelling is expected, especially if the resective technique has been used and required extensive dissection. The catheter should remain in place for 48hours.
Antibiotic therapy: Based on culture results or empirical impression, antibiotic treatment should be continued for a minimum of 2 weeks after surgery. If evidence of pyelonephritis is present, antibiotic therapy should be continued for 6 to 8 weeks.
Pain management: Administer nonsteroidal antiinflammatory drug(s) for 1 week and narcotics for a few days after surgery.
Incontinence after surgery: Repeat diagnostics to rule out contralateral EU.
Alpha-adrenergic agents: Prescribe phenylpropanolamine (1.5–2.2 mg/kg PO Q 8-24 H) or ephedrine sulfate (1–4 mg/kg PO Q 8-12 H) if urinary continence is not achieved and no other problems can be found.
Urethral bulking injections: See Urethral Bulking Procedures, page 61.
Colposuspension
In addition to corrective surgery to reposition the opening of the EU into the bladder, the sphincter region of the bladder may be tightened using the colposuspension technique. Generally, about 50% of dogs will be continent with the corrective ureteral surgery and, in refractory cases, with the addition of phenylpropanolamine. In a small series of EU cases, urinary continence was achieved in 71% of cases that received corrective ureteral surgery and colposuspension.
This procedure involves retracting the vagina cranially and placing 2 horizontal mattress nonabsorbable sutures, such as 0 to 2-0 polypropylene, through the left and right prepubic tendons and the ventrolateral vaginal walls. After the sutures have been tied, only a small finger should be able to be passed between the ventral abdominal wall and the vagina.

Urethral Bulking Procedures
If the patient is still incontinent despite surgical procedures being performed, a bulking agent can be injected (using a cystoscope) intothe wall of the urethra at the level of the internal urinary sphincter. Because commercial production of injectable collagen has beendiscontinued, some veterinarians are starting to use silicon (polydimethylsiloxane). Long-term results using this product are not available.
Hydraulic Constrictor
Because dogs may still be incontinent after EU surgery, some surgeons will prophylactically place a hydraulic constrictor around the proximal urethra at the time of EU correction. This device is gradually inflated over a period of weeks until urinary continence is achieved. Although no published data are available, some surgeons have had successful outcomes with the use of this device. However, in some cases a serious complication of progressive irreversible stricture of the urethra has been seen.
Author Insight
Patients refractory to standard treatments may benefit from placement of a hydraulic constrictor around the urethra.