This response is incorrect. See below for the correct answer.
Top 5 Masses Diagnosed With In-House Cytology
Katie M. Boes, DVM, MS, DACVP, Virginia–Maryland College of Veterinary Medicine

Cytology, a relatively noninvasive means for rapid in-clinic diagnosis, can be useful for identifying sampled masses, fluids, or lesions, frequently without undue patient harm.
Fine-needle aspiration of internal lesions may require ultrasonographic assistance and confirmation of normal coagulation status (eg, clotting times, platelet numbers). Skin cytology samples can be acquired via fine-needle aspiration, impression smear, or skin scrape, all of which have few clinical complications. For some masses, cytologic features can be difficult to interpret, but general practitioners should be able to confidently diagnose several common skin masses with cultivation of cytologic and microscopic skills.
1. Vaccine reaction
Vaccine reactions may occur at vaccination sites weeks or months following administration. On cytologic examination, there is a mixed inflammatory infiltrate of mostly lymphocytes and macrophages with some plasma cells, neutrophils, and eosinophils. Macrophages become activated with increased cytoplasmic basophilia, foamy cytoplasm, binucleated forms, and multinucleated giant cells. The key diagnostic feature is macrophages containing phagocytized adjuvant (visualized as a bright pink, purple, or blue globular or granular material; Figure 1). If inflammation is not self-limiting and the mass does not resolve, complete surgical excision should be curative.
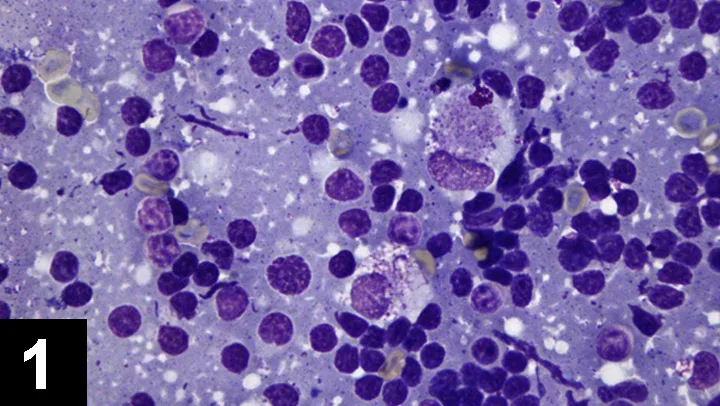
Fine-needle aspirate of skin from a dog with vaccine reaction showing many small lymphocytes and 2 activated macrophages that have phagocytized a purple, granular material (vaccine adjuvant) admixed with a few lysed lymphocytes. (Diff-Quik stain, 1000× original magnification)
2. Follicular cyst
Follicular cysts (ie, epidural inclusion cysts, epidermoid cysts) are nonneoplastic, noninflammatory, sac-like lesions lined by epithelium. Most canine and feline skin cysts are follicular cysts (ie, arise from hair follicles) and include several histologic subtypes that are not cytologically distinguishable. These histologic subtypes have little clinical significance; they are benign and can be completely excised surgically.
On cytologic examination, follicular cysts have abundant keratinocytes (either anucleate or containing karyolytic nuclei) with cholesterol crystals, hair fragments, and activated macrophages (Figure 2). Within the preparation background, follicular cysts can also contain melanin granules that should be differentiated from bacteria. Cyst rupture and immunogenic keratin exposure to the dermis or subcutis can result in foreign body reaction with mild-to-marked infiltrates of neutrophils, macrophages, and multinucleated giant cells. Because, on cytology, a cyst cannot be differentiated from a cyst within a neoplasm (usually benign follicular neoplasm), histopathology is required to assess architecture; cytologic differentials include trichoepi- thelioma, infundibular keratinizing acanthoma, and pilomatrixoma.
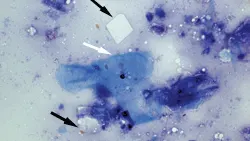
Fine-needle aspirate from a follicular cyst in the skin of a dog showing a few hyalinized, moderately basophilic, angular keratinocytes (white arrow) and 2 colorless, rectangular-to-rhomboidal cholesterol crystals (black arrows). (Modified Wright stain, 1000× objective field)
3. Lipoma
Lipomas, benign neoplastic adipocyte growths, are typically soft, freely movable masses of varying sizes within the subcutis; however, infiltrative lipomas may be firmer and attached to underlying musculature. Before staining, lipoma preparations appear greasy and fail to air-dry. During staining, adipocytes may dissolve in the fixative to produce an acellular cytologic sample. If they do not completely dissolve in the fixative, adipocytes appear as large balloon-like cells arranged in aggregates held together by fine fibrovascular stroma (Figure 3). Individual cells are round to polygonal and contain a large, colorless intracytoplasmic vacuole that peripherally displaces a small, round, condensed nucleus. Complete surgical excision, if permitted by owners, can be curative.
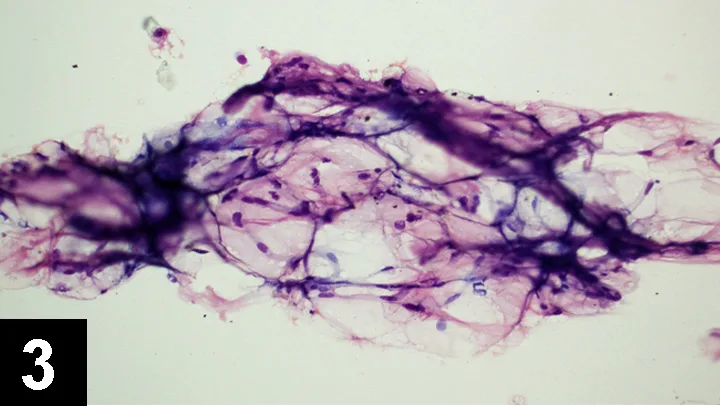
Fine-needle aspirate from a lipoma in the skin of a dog showing a large aggregate of balloon-shaped adipocytes held together by a fine fibrovascular stroma. (Modified Wright stain, 200× objective field)
4. Histiocytoma
Canine histiocytomas are benign, self-limiting dermal growths that usually occur on the ears, face, and distal extremities of young dogs. Histiocytomas can also occur in older dogs, but other tumors (eg, other round cell tumors) should be considered. These lesions are frequently erythematous, alopecic, and dome-shaped with or without ulceration. On cytologic examination, many individualized, (irregularly) round histiocytes may display minimal or mild anisocytosis and anisokaryosis and contain some lightly basophilic cytoplasm that often stains paler than the platform background and is paler at the periphery as compared with that evident on perinuclear staining. A few punctate, colorless vacuoles may be noted. Nuclei are round to ovoid, variably placed in the cell, and display lacy chromatin with absent or occasional nucleoli (Figure 4). Varying numbers of small lymphocytes may be dispersed with increased lymphocyte numbers observed in regressing histiocytomas. Because histiocytomas cannot be cytologically differentiated from cutaneous or systemic histiocytosis, the latter conditions should be considered in dogs with multiple histiocytoma-like skin lesions.
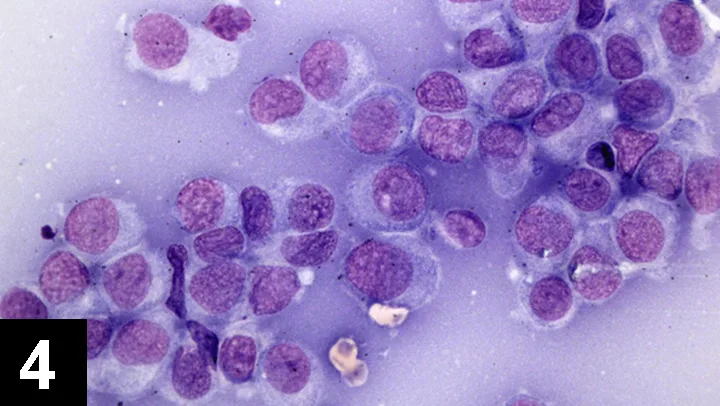
Fine-needle aspirate from a histiocytoma in a dog’s skin showing many round histiocytes with mild anisocytosis and anisokaryosis and containing a moderate amount of lightly basophilic cytoplasm. The nuclei are round with lacy-to-stippled chromatin and 0 or 1 nucleolus. (Modified Wright stain, 1000× objective field)
5. Mast cell tumor
Canine mast cell tumors may be solitary or multicentric in the skin and can appear sequentially or simultaneously. They tend to be alopecic, erythematous, and varied in size. Ulceration may be present in larger masses, and the mass may change size as histamine is sporadically released from the neoplastic cells. On cytologic examination, these tumors frequently contain several mast cells and eosinophils with fewer neutrophils, fibroblasts, and collagen strands. Mast cells are round and individualized and contain lightly basophilic cytoplasm with few-to-numerous deeply basophilic intracytoplasmic granules (Figure 5A). The degree of granularity depends on the granule’s staining characteristics, stain type, degree of cellular differentiation, and whether mast cells have recently degranulated in situ.
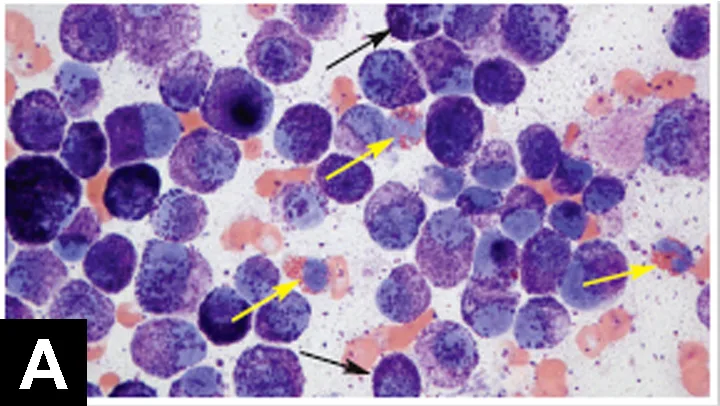
Three eosinophils (yellow arrows) and multiple mast cells (black arrows) with numerous intracytoplasmic, deeply basophilic granules and round, pale-staining nuclei. (Modified Wright stain, 1000× objective field)
Often, the granules are so numerous that they physically obscure nuclear features or absorb so much stain that the nucleus stains pale. In contrast, some aqueous-based Wright stains (eg, Diff-Quik) stain poorly or fail to stain the granules (Figure 5B). If the granules do not stain, diagnosis can be achieved by observing eosinophils admixed with individualized round mast cells that display round, centrally placed nuclei and foamy or vacuolated cytoplasm. Any mast cell tumor should be considered potentially malignant, but greater nuclear pleomorphism (ie, anisocytosis, binucleation) and observation of mitotic figures should increase concern for malignancy. Canine mast cell tumors should be surgically removed with wide margins (3 cm or 1 fascial plane) and submitted for histopathologic evaluation and grading.
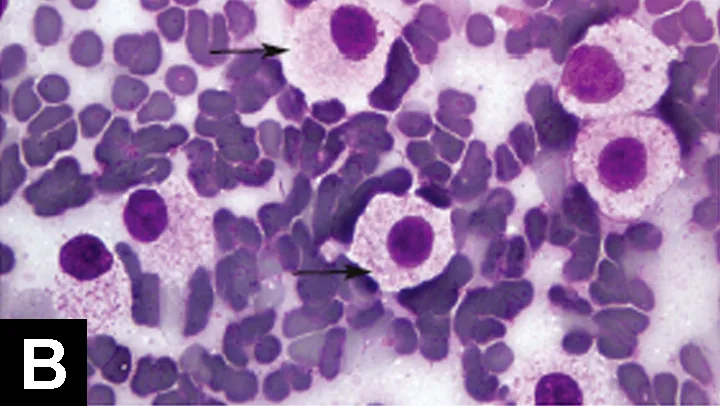
Poorly stained mast cells (arrows) with few lightly basophilic intracytoplasmic granules. (Diff-Quik stain, 1000× objective field)
Closing thoughts
More challenging preparations can be sent to diagnostic laboratories for pathologist review, but several neoplastic and nonneoplastic lesions, such as those listed here, can be evaluated in-house to facilitate faster diagnosis and treatment.