Step-by-Step Cystotomy
Eric R. Pope, DVM, MS, DACVS, Ross University
Indications for cystotomy include exploration of the lower urinary tract, removal of cystic and urethral calculi (Figure 1), correction of ectopic ureters, removal of masses (eg, polyps), and biopsy.
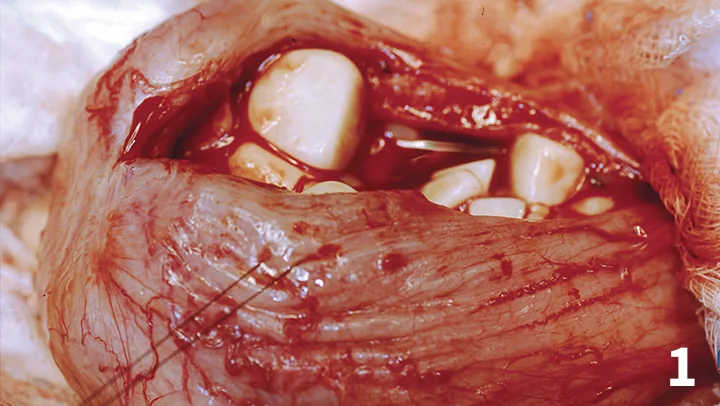
Cystotomy for multiple cystoliths.
Cystotomy can be completed via 1) an open approach via midline celiotomy or 2) a limited caudal midline approach in conjunction with cystoscopy or urethroscopy. Although the limited approach may be less invasive, total costs are often higher than with the more traditional open approach, and specialized equipment is required.1 Cystotomy via ventral midline celiotomy may be the most common approach in general practice.
Positioning & Location for Cystotomies
Cystotomy is conducted with the patient in dorsal recumbency. Male dogs can be positioned with the pelvic limbs extended caudally because the prepuce can be included in the prepared field should urethral catheterization be necessary. Placing the pelvic limbs of female dogs and cats in so-called “frog-leg” position with the tail hanging over the surgery table can provide good access for normo- or retrograde urethral catheterization intraoperatively; this positioning also works well in male cats when cystotomy is combined with either urethral catheterization or perineal urethrostomy.
The ventral abdomen should be clipped and aseptically prepared from the xiphoid to the caudal aspect of the pubis. The perineum can also be included in the preparation. The prepuce and vulva should be flushed with antiseptic solution (eg, 0.05% chlorhexidine solution) surgically prepared and included in the field to facilitate intraoperative catheterization.
In cats and female dogs, a ventral midline celiotomy is performed from just caudal to the umbilicus to the cranial brim of the pelvis. In male dogs, a parapreputial skin incision is used. Ligation or electrocoagulation of the preputial branches of the caudal superficial epigastric vein and subcutaneous vessels minimizes bleeding. Transect the preputial muscle, retract the prepuce to the opposite side, and perform a midline celiotomy. The preputial muscle can be tagged with suture to identify it during closure.
Although a cystotomy can be performed on the dorsal or ventral surface of the bladder,2 a ventral midline cystotomy is recommended. Ventral cystotomy provides excellent visualization of the bladder lumen—especially the trigone area—and can be extended into the proximal urethra if additional exposure is necessary.
Catheterization
The bladder becomes thickened and edematous with prolonged exteriorization and repeated manipulations. Stay sutures can reduce repeated grasping of the bladder. The urethra can be catheterized normograde (from bladder to urethral orifice), retrograde (from urethral orifice to bladder), or in both directions to verify patency and to flush calculi, when present, from the urethra. Placement of an indwelling urethral catheter in small female dogs and female cats can be facilitated by passing a catheter normograde from the bladder, attaching it to the tip of a second catheter, and withdrawing the normograde catheter to pull the indwelling catheter through the urethra and into the bladder if retrograde placement is difficult.
On Sutures
Simple interrupted, simple continuous, simple continuous oversewn with an inverting pattern (eg, Cushing), single layer Cushing pattern, and Cushing pattern oversewn with the Lembert pattern have all been used.2-5 Inverting patterns should be avoided when the bladder wall is thickened or friable.
The simple continuous pattern can be used in normal or thickened bladders. A simple continuous pattern engaging the seromuscular layers and submucosa, while avoiding the mucosa, should be placed. Suture bites should be 3 mm to 4 mm apart with similar distance between sutures. In normal bladders, the simple continuous pattern can be oversewn with a Cushing pattern at the discretion of the surgeon, but there is no demonstrated benefit over a single-layer closure.4 If an inverting pattern is used, take care to avoid excessive inversion of tissue, which could result in obstruction.
A monofilament intermediate lasting absorbable suture material such as poliglecaprone 25 (ie, Monocryl) or glycomer 631 (ie, Biosyn) in size 3/0–5/0 on a taper point needle works well. Resistance should be felt when the submucosa is engaged.
Follow-Up
The bladder can be filled with saline to check for leaks. Simple interrupted or cruciate suture(s) to seal leaks should be placed. The surgery site should be lavaged with warm sterile saline before routine closure of the abdominal wall. In male dogs, the transected preputial muscle should be sutured. When cystotomy has been performed for cystolith removal, postoperative radiographs or other imaging appropriate for the stone type should be performed to confirm complete removal of the stones from the bladder and urethra. There is a relatively high frequency of stones being left behind even when the bladder and urethra are extensively flushed during surgery.7
Monitor urine output and appearance (eg, hematuria) postoperatively. Continue fluid administration as long as blood clots continue to pass to reduce the risk of obstruction. Control pain with opioids perioperatively. In cats, transmucosal (placed in buccal pouch) buprenorphine typically works well. In dogs, continue NSAIDs for 3 to 5 days for their anti-inflammatory and analgesic effects as long as the patient is well-hydrated and renal function is normal. A single post-operative dose of an NSAID can be considered with the previously mentioned precautions.
Complications
Complications after cystotomy are uncommon, but the patient should be monitored for evidence of dehiscence (Figure 3), infection, persistent hematuria, excessive stranguria, and obstruction (see Important Considerations in Cystotomy Closure). Dehiscence or suture line leakage is the result of infection, inadequately placed sutures, or increased intravesicular pressure secondary to impaired urine outflow.
Important Considerations in Cystotomy Closure
Many suture patterns and techniques have been used for successful urinary bladder closure. Essential key points to minimize complications are:
The urinary bladder heals quickly, typically achieving 100% of normal strength in 3 weeks.2-4
Sutures should engage the submucosa, which is the layer of strength.2,4,5
Apposition of like layers results in a rapid gain in wound strength and does not reduce lumen size4
Minimal to no suture material should penetrate the lumen,2-5 especially in patients with chronic or recurrent urinary tract infections that could be predisposed to calculogenesis3 (Figure 2).
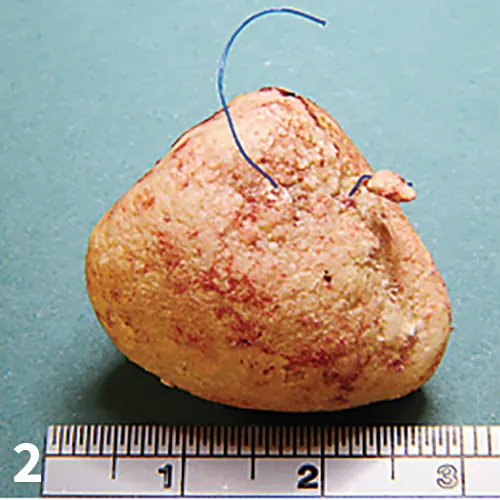
Suture removed from lumen of the bladder of a dog with history of multiple cystotomies for cystolith removal associated with urinary tract infections.
The closure must be watertight and strong enough to withstand pressures generated during micturition.3
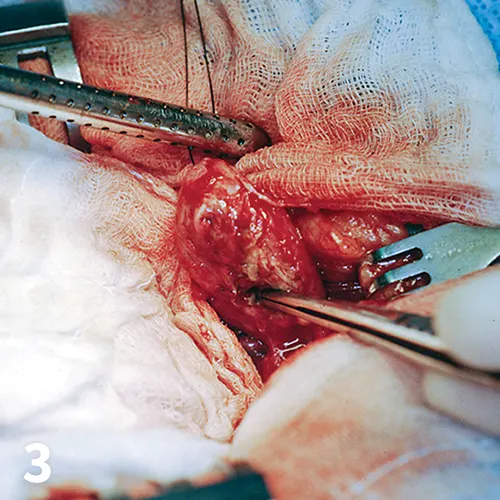
Exploration of a dog with uroperitoneum after closure of ruptured urinary bladder with a simple continuous pattern.
Step-by-Step: Cystotomy
What You Will Need
General surgery pack (ie, scalpel handle, DeBakey thumb forceps, needle holders, Metzenbaum scissors, hemostats)
Balfour or similar abdominal retractors
Surgical and laparotomy sponges
Red rubber or similar soft catheters for urethral or ureteral catheterization
3/0 or 4/0 nylon for stay sutures
3/0 – 5/0 monofilament absorbable suture material on a taper point needle for cystotomy closure
Poole or similar suction tip
Formalin containers for biopsy specimens
Sterile cup or culture swab and medium for transporting mucosal biopsies and/or small stones for culture
Warm sterile saline for lavage
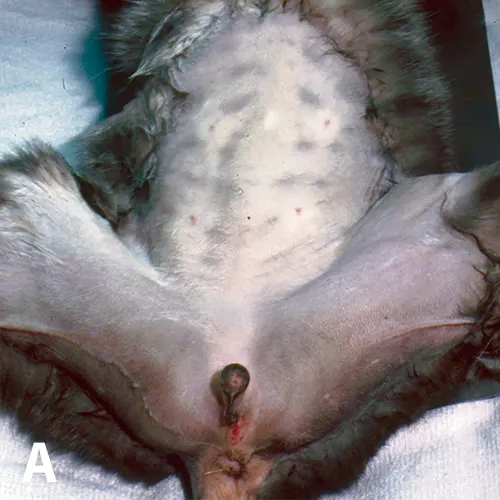
STEP 1A.
Position the patient in dorsal recumbency. Pictured is a cat with recurrent urethral obstruction and calcium oxalate uroliths (A).
Author Insight
Perform cystotomy on ventral aspect of bladder for better exposure of the trigone area.