Spotted Fever Rickettsiosis in Dogs: An Update
Profile
Definitions. Spotted fever group (SFG) Rickettsia are small, vector-borne, obligately intracellular bacteria. There are more than 20 species belonging to this group and most have been discovered recently. SFG Rickettsia are important causes of emerging infectious disease in people.1
Rickettsia rickettsii, the cause of Rocky Mountain spotted fever (RMSF) and R conorii, the cause of Mediterranean spotted fever, have been shown to infect and cause disease in dogs.2,3 In addition, dogs are sentinels for R rickettsii and R conorii infection in people.4-6 Canine RMSF is well characterized and the focus of this article; however, veterinarians should be aware that infection with novel species in dogs is likely.
Related Article: Practical Guide to Tick-Borne Disease
Incidence/Prevalence. The incidence of rickettsioses in people is increasing due to disease caused by species previously thought to be nonpathogenic, new forms of disease caused by recently discovered species, and spread into nonendemic regions by novel vectors. Human RMSF is a reportable disease in the U.S. Counties in some states also require reporting for dogs, particularly during suspected outbreaks. Signs of illness may become evident in dogs before or coinciding with infection in people living in the same household, and exposure can be detected in dog populations before human epidemics.4,5,7 Veterinarians, therefore, play a pivotal role in preventing illness in both dogs and people.
Geographic Distribution.The geographic distribution of RMSF is expanding.
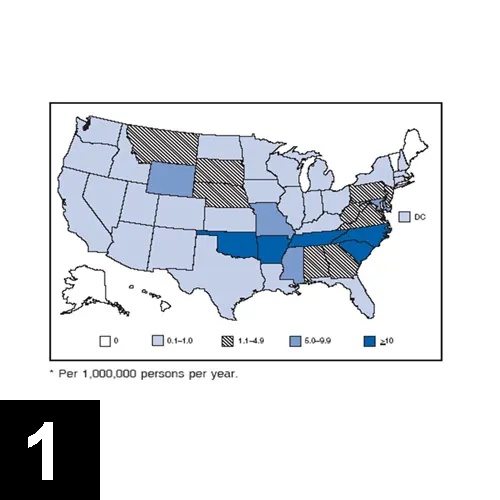
Historically, most cases occur in the southeast and south central U.S. (Figure 1). Disease distribution followed the primary vectors, Dermacentor variabilis and D andersonii. However, Rhipicephalus sanguin_eus, a tick that normally prefers to feed on dogs and is ubiquitously distributed, caused a recent outbreak of RMSF in people in a nonendemic area of Arizona.8 Furthermore, other tick species in the U.S. are also infected with _R rickettsii. Veterinarians practicing in nonendemic areas should be vigilant for disease caused by novel tick vectors.9
SignalmentYoung and purebred dogs are overrepresented in some studies. Severe disease may occur in English springer spaniels with phosphofructokinase deficiency and in German shepherd dogs. No sex predilection has been definitively documented.3,10
Risk FactorsAlthough disease can occur any time of year, most cases of RMSF are reported from April through October, months of peak tick activity. Dogs living outdoors are at increased risk.3,10
Related Article: Ehrlichiosis in Dogs
PathophysiologyTick feeding activates the organism, which is transmitted in saliva. Because the organism infects endothelial cells, clinical signs are consistent with vasculitis-manifesting as disordered primary hemostasis, edema, and microthrombosis. Thrombocytopenia is common due to vasculitis and immune-mediated platelet destruction. Low numbers of organisms circulate in blood for a short period of time after infection (13 days). This period corresponds to the time that clinical signs are observed.11,12 Accordingly, RMSF is an acute disease; chronic infection has not been documented in dogs. Antibody titers may be long-lived, and immunity to infection is likely lifelong.
Signs
A range of signs can occur that may be nonspecific.
History. Often, there is no known history of a tick bite. Lethargy and anorexia are common and can be the only presenting complaints. Vomiting and diarrhea may be reported. Melena may be observed, as well as various central nervous system (CNS) abnormalities, including vestibular disease and seizures. Dramatic and rapid weight loss has been described.3,10,13
Physical Examination.
Fever is often present, but not always.
Ocular signs are frequently observed, and may include discharge, scleral and conjunctival injection and hemorrhage, conjunctivitis, uveitis, retinal hemorrhage, and retinitis
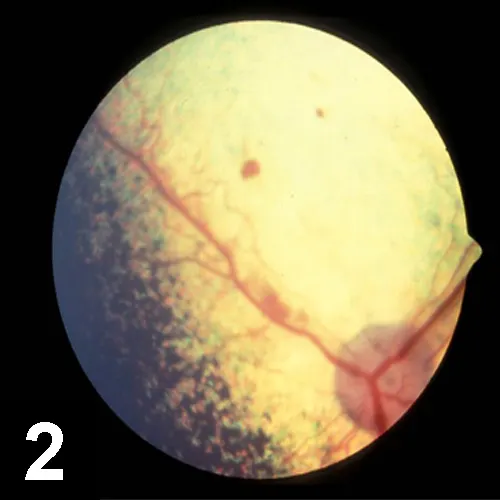
(Figure 2).* Lymphadenomegaly is common.
Respiratory abnormalities include nasal discharge, epistaxis, tachypnea, and dyspnea.
Mucocutaneous and cutaneous abnormalities include petechiae, ecchymosis, edema, hyperemia, and necrosis.
Orchitis and scrotal edema, hyperemia, and epididymal pain are common in intact dogs.
Generalized myalgia and arthralgia can be observed.
CNS abnormalities, which can be focal or generalized, include hyperesthesia, ataxia, vestibular signs, stupor, seizures, and coma.
Arrhythmias may be noted.
Microvascular hemorrhage, thrombosis, hypotension, oliguric renal failure, cardiovascular collapse, and brain death occur terminally.3,10,13
Diagnosis
A high index of suspicion based on clinical signs is necessary because treatment must be instituted before definitive diagnostic tests confirm infection.3,11
Differential Diagnosis
Infection with other tick-borne agents (eg, A phagocytophilum; Ehrlichia, Bartonella, and Babesia species; Borrelia burgdorferi)3
Sepsis, systemic inflammatory response syndrome (SIRS)
Leptospirosis
Other causes of vasculitis and thrombocytopenia
Other causes of CNS disease
Laboratory Findings(Most frequently encountered findings are marked with an asterisk.3,13)
Thrombocytopenia most common (83% of patients)*
Leukocytosis (neutrophils may have toxic change)*
Nonregenerative anemia
Hypoalbuminemia*
Elevated alkaline phosphatase*
Hyponatremia
Hyperbilirubinemia
Coagulation abnormalities
Prolonged prothrombin time
Prolonged activated partial thromboplastin time*
Elevated fibrinogen*
Elevated fibrinogen degradation products
Disseminated intravascular coagulation (uncommon)
Proteinuria
Hematuria*
Bilirubinuria*
Pyuria
Mixed-cell pleocytosis
Neutrophilic polyarthritis
Imaging
Findings depend on organs involved.
Thoracic radiographs may show an unstructured interstitial pattern.
Diagnostic TestsGeneral considerations:
Handle specimens with care and mark clearly as biohazards.
Contact with or aerosolization of rickettsemic blood should be avoided.
Most tests do not differentiate among species of SFG Rickettsia:
Species presumed based on geographic locale (eg, seropositive patients are presumed to be infected with R rickettsii in the western hemisphere).
Other species of SFG Rickettsia are present in the United States.14
Novel species will not be recognized with routine diagnostic testing.
Serology
Microimmunofluorescence
Microimmunofluorescence testing of acute and convalescent samples documenting a fourfold change in titer is the gold standard for diagnosis.
Do not rule out diagnosis based on asingle negative titer.
Can be negative acutely3,11
Clinical signs can occur before seroconversion.
A positive titer does not confirm active infection.
Antibodies cross-react among other SFG Rickettsia.
Exposure to other nonpathogenic (or less pathogenic) Rickettsia symbionts of ticks is common.14,15
Cross-reactivity occurs in dogs and people infected with Bartonella henselae.16
Previous infection with R rickettsii can result in long-lived antibody titers.11,17
Polymerase Chain Reaction (PCR)
PCR can be used to detect infection in some acutely infected seronegative dogs.
Negative PCR does not rule out infection; low numbers of organisms circulate for a short period of time.
A sensitive PCR that detects and differentiates among SFG Rickettsia infecting dog blood has been described.18
Studies regarding the sensitivity and specificity of other PCR assays used in dogs have not been published.
Immunohistochemistry/Gimenez Staining
Can confirm infection using tissue samples.
Does not differentiate species.
Treatment
Inpatient or OutpatientMost patients require hospitalization.
Medical TherapyThe general medical approach to therapy is outlined in Medications.
Inappropriate antibiotic therapy may increase morbidity and mortality.3 The use of trimethoprim-sulfamethoxazole may even worsen the disease. Delaying therapy also increases the risk for complications; therefore, therapy must begin based on clinical suspicion before diagnostic tests confirm infection. Aggressive supportive care for complications such as DIC and thrombosis may be necessary. Cautious use of fluids and colloids may be warranted in some cases; however, avoid exacerbation of edema.
Medications
AntibioticsDoxycycline(5 mg/kg PO Q 12 H for 7-14 days)
Treatment of choice
Parenteral administration may be necessary transiently in debilitated patients or those with vomiting.
Effective empiric therapy for A phagocytophilum, B burgdorferi, and Ehrlichia infections (differential diagnoses for RMSF)
Coinfection may require a longer treatment course.
Theoretical risk for tooth discoloration in puppies not well documented.
Chloramphenicol(15-30 mg/kg PO Q 8 H for 7-14 days)
Effective in experimentally infected dogs
Parenteral administration may be necessary transiently in debilitated patients or those with vomiting.
May be less effective than doxycycline for treating RMSF in people, and less effective against E chaffeensis and A phagocytophilum (differential diagnoses for RMSF) than doxycycline (in vitro)19
Has been suggested for use in infected puppies, but caution is warranted.
Adverse side effects
Bone marrow suppression
Risk to humans: Aplastic anemia (wear gloves)
Enrofloxacin(5 mg/kg PO Q 12 H for 7-14 days)
Effective in experimentally infected dogs
Not for use in young animals (cartilage abnormalities)
Not effective against E canis (differential diagnosis for RMSF)20
Corticosteroids
Controversial; antiinflammatory and immunosuppressive doses did not affect outcome but rickettsemia was prolonged in sublethally experimentally infected dogs.21
Antiinflammatory doses have been used in dogs with severe CNS manifestations and may also be necessary in dogs with ocular abnormalities.<sup13, 22sup>
Follow-Up
Response to appropriate antibiotic therapy is very rapid (24-48 hours).
Coinfection with B burgdorferi, E canis,E ewingii, E chaffeensis, Babesia canis, and Bartonella species should be considered in dogs with severe or prolonged clinical signs.3
Residual CNS and other deficits may occur in severely affected patients.
Convalescent titers should be drawn 2 to 3 weeks after initial sample.
PrognosisThe prognosis for dogs with RMSF is good to excellent if diagnosed and treated with appropriate antibiotics and supportive care early.3,13
In General
Relative CostDiagnostic workup and treatment: $-$$
Client Education
Communicate with owners and physicians that infections in dogs may precede tick-transmitted infection in owners.
Instruct clients to remove ticks properly and avoid crushing to prevent exposure to infected hemolymph
Educate regarding use of tick control and prevention for owners and pets
Future ConsiderationsNovel and well characterized species of SFG Rickettsia are important causes of emerging infectious disease in dogs and people. Furthermore, R rickettsii is considered a potential bioterrorist agent.22 Because dogs are sentinels for infection, veterinarians can play an important role in detecting, defining, and preventing illness in their canine patients and their human companions.