Rostral Mandibular Mass in a Dog
Sarah Boston, DVM, DVSc, DACVS, ACVS Founding Fellow of Surgical Oncology, ACVS Founding Fellow of Oral & Maxillofacial Surgery, VCA Canada, Newmarket, Ontario, Canada

Fleshy mass of the rostral mandible of the patient
History
An 11-year-old, neutered male boxer was referred with an oral mass of several weeks duration. No other clinical signs were present.
Physical Examination
General physical examination revealed no abnormalities. Vital signs were within normal limits. Oral examination disclosed a firm, fleshy mass 2.5 cm in diameter on the rostral mandible at the level of the incisors (Figure 1). Palpation of the mandible elicited no apparent pain. Except for 103, all lower incisors were missing or could not be visualized.
Related Article: Common Oral Tumors in Dogs & Cats
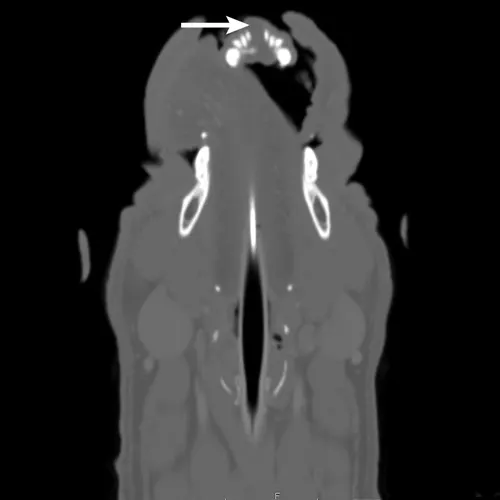
Axial CT image of the head showing an oral mass (arrow) of the rostral mandible. Note the mild lysis of the mandible and widening of the interdental space between the left and right mandibular first incisors.
Diagnostics
CBC and serum chemistry profile were within normal limits. Three-view thoracic radiographs were negative for metastatic disease. The patient was anesthetized, and CT of the head and thorax and an incisional biopsy were pursued in the same anesthetic period. The CT scan showed a well-defined, 2.2 x 2.5 x 1.4-cm noncontrast-enhancing, soft-tissue–attenuating mass on the rostral dorsal aspect of the mandible at the level of the incisor teeth, with mild lysis of the mandible and widening of the interdental space at the mandibular symphysis (Figures 2 and 3). The mandibular and retropharyngeal lymph nodes (the most important lymphatic centers for a tumor in this region) and other lymph nodes of the head and neck appeared normal.
The surgeon used an intraoral approach to obtain a wedge biopsy from the center of the mass. The tissues around the mass were undisturbed, and the oral mucosa was closed using 3-0 PDS in a simple interrupted pattern.
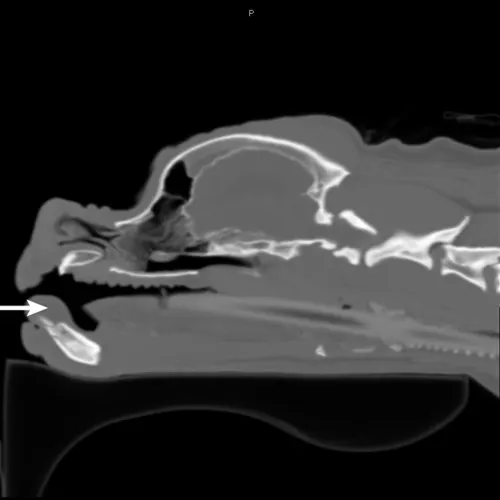
Sagittal CT image of the head showing an oral mass (arrow) of the rostral mandible
Diagnosis
Histopathology of the incisional biopsy specimen was consistent with an acanthomatous ameloblastoma, a tumor that often has locally invasive behavior but does not have metastatic potential.1,2
Surgery is the gold standard treatment for a small tumor with a rostral location.
Treatment
Treatment options, including surgery and radiation therapy, were discussed with the owner. Although radiation therapy can effectively treat a tumor in the mandible, surgery is considered the gold standard treatment for a small tumor with a rostral location. Surgery is more likely to provide local control with the shortest treatment period, and the cost is approximately half that of radiation therapy.1 Radiation therapy may also cause mucositis, which can be markedly painful, in the oral cavity.2 Intralesional bleomycin has also been used to treat this tumor type and may lead to long-term control.3
The following week, the patient underwent wide excision of the mass with 2-cm margins based on the visible tumor mass and CT scan findings.
Related Article: Nerve Blocks for Oral Surgery in Dogs
Cross-match and blood typing were performed preoperatively, and a mandibular nerve block was administered bilaterally before the procedure. The surgeon used an oscillating bone saw to perform a bilateral rostral mandibulectomy (Figures 4 and 5). For closure, the gingival mucosa was attached to the lingual mucosa with an absorbable suture in a simple continuous suture pattern. A triangle of skin was excised from the midline to remove redundant tissue from the chin. Subcutaneous tissue was closed over the ends of the mandible to prevent protrusion through the closure. The skin was closed maintaining the continuity of the mucocutaneous junction.

Figure 4 Preoperative positioning of the patient in dorsal recumbency. Pharyngeal swabs have been placed to prevent aspiration of blood; blue synthetic fibers assist with removal of swabs.
The patient recovered without incident and was admitted to the ICU for supportive care with IV fluids and meloxicam (0.1 mg/kg IV once a day) and hydromorphone (0.1 mg/kg IV every 4-6 hours) for pain control. The surgical margins were inked, and the entire specimen was submitted for histopathology and margin assessment (Figure 6). Histopathology confirmed acanthomatous ameloblastoma. The margins of excision were considered clean, with no evidence of tumor cells within >10 mm of the inked surgical margins.

The patient at suture removal 12 days postoperatively
Outcome
The patient was eating soft food within 24 hours of surgery and was discharged 48 hours postoperatively. The owner was advised to feed the patient canned food, as well as avoid offering toys or hard treats, for 1 month.
At suture removal 12 days postoperatively, the patient showed no abnormalities and was eating without difficulty. Cosmesis and function were considered excellent (Figure 7).