Respiratory Distress in a Pug

A 10-year-old, spayed, female pug is presented for respiratory problems.
History. The owner reported a combination of chronic cough and inspiratory dyspnea. Coughing had begun 10 months previously. The cough was described as intermittent, dry, honking, and partially responsive to hydrocodone and antibiotics. It became worse in the early summer, leading to the addition of diphenhydramine. Over the past few months, the cough had subsided, but the owner noticed difficult, noisy inspirations. Hot weather greatly exacerbated the condition. At presentation, medications were hydrocodone, prednisolone (1 mg twice a day), theophylline, and diphenhydramine.
Examination. The dog was alert and responsive but panted continuously. Marked inspiratory dyspnea with stertor was noted; mucous membranes were pink and capillary refill time was less than 2 seconds. Thoracic auscultation was impossible due to loud, referred, upper-airway sounds. A cough could not be induced. Body temperature was 103.4º F, body weight was 10 kg, and body condition score was 5/5. The liver was palpably enlarged. Marked dental disease was present.
Laboratory Results. Unremarkable except for increases in ALP (3 times the normal level) and ALT (1.5 times the normal level) attributed to long-term steroid therapy. Pulse oximetry result was 93%.
Radiographs. Survey radiographs of the thorax (Figure 1) demonstrate morbid obesity. No significant abnormalities are noted in the lung fields, although assessment is difficult due to obesity, thoracic conformation, and poor inspiration. There is variation in the tracheal diameter in the cervical region. The cardiac silhouette is unremarkable.
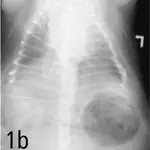
Right lateral (a) and dorsoventral (b) views of the thorax demonstrating severe obesity and variation in the tracheal diameter in the cervical region. The cardiac silhouette and lung fields are unremarkable.
Fluoroscopic examination demonstrates thickening of the soft palate, without evidence of elongation, and thickening of the retropharyngeal tissues with near-total obliteration of the naso- and oropharyngeal air passages during inspiration. The patient's cervical trachea shows moderate variation in diameter during respiration. A cough could not be induced during this procedure.
Sedated Oropharyngeal Examination. Limited visualization due to narrow oropharyngeal diameter. No evidence of mass or other pathologic process of the oropharyngeal tissues.
ASK YOURSELF...Which of the following is the optimal therapeutic approach for this dog?A. Counsel owner regarding weight reduction, and schedule recheck for respiratory signs once weight loss has begun.B. Institute more aggressive medical management for chronic bronchitis to reduce severity of lower airway disease and cervical tracheal collapse.C. Treat for pharyngeal/laryngeal edema with high-dose steroids.D. Reduce inspiratory dyspnea and pharyngeal collapse by surgically treating the dog for brachycephalic syndrome (stenotic nares, everted lateral saccules, and elongated soft palate).E. Refer for surgical placement of a tracheal stent for tracheal collapse.
Correct Answer: ACounsel owner regarding weight reduction, and schedule recheck for respiratory signs once weight loss has begun.
The most likely cause of this dog's dyspnea is pharyngeal narrowing. The lack of coughing as a current sign as well as modest collapse in the cervical tracheal region only suggest that collapsing trachea is not the primary problem to address. Therefore, more aggressive medical management for chronic bronchitis or surgically stenting the trachea (a last-resort procedure for predominantly intrathoracic tracheal collapse) is not indicated. The signs are chronic, and oral examination failed to reveal any evidence of pharyngeal or laryngeal edema.
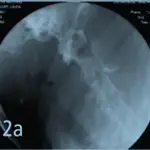
Although surgically addressing an elongated soft palate (and concurrent abnormalities) might be helpful in some brachycephalic dogs, in this dog the soft palate appeared to be thickened but not elongated (Figure 2). Surgery would probably worsen the dog's respiratory distress, perhaps necessitating placement of a tracheostomy tube. Weight loss to decrease fat deposits around the neck and face and to alleviate the "Pickwickian" syndrome is the safest approach to initial management of this stable patient.
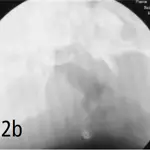
Lateral radiograph (2a) of the pharynx demonstrating extreme thickening of the soft palate, without evidence of elongation. The retropharyngeal tissues are also thickened. The naso- and oropharyngeal air passages are nearly obliterated. For contrast, a similar lateral view of the pharynx of another brachycephalic dog is shown in Figure 2b.
In this case, the owner was counseled about the health consequences of morbid obesity for her dog. A weight reduction program resulted in a 3-kg weight loss (almost 1/3 of body weight) over 4 months.
The owner was advised to try to wean the dog off steroids. With weight loss, the dog's respiratory signs improved significantly, and it became more tolerant of environmental temperature variations as well as light exercise.
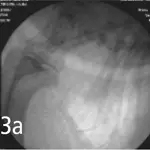
Figure 3. Spot films from fluoroscopic study demonstrating maximal change in tracheal diameter that occurred in this dog. A cough could not be induced during this procedure.
How to Implement a Weight-Loss ProgramIdeally a weight-loss program should have three components: 1) owner commitment, 2) customized program for the patient and family, and 3) regular monitoring.1. Ensure that the owner and family are committed to weight reduction in their pet. Educate about the potential health risks and health care costs associated with obesity.
2. Assess the animal: Rule out/treat contributing or associated diseases. Estimate target (ideal) body weight.
3. Assess current food intake: Take a thorough diet history. Consider having owner complete 3-day food journal if several types of dog food or "people" foods comprise a significant portion of the diet. Include foods used to give medications. From this information, estimate current daily intake of calories.
4. Decide how much caloric restriction to impose for weight reduction: Feed 60% to 70% of the current daily caloric intake (preferred method). If intake is extraordinarily excessive, this strategy may be ineffective in producing weight loss. If so, see below.orCalculate energy requirement at the dog's ideal weight (if current intake is not available and/or not credible). Feed 60% of the goal energy requirement: 60%[1.4 (30 × BWkg + 70)] The dog should not lose more than 4% body weight per week.
5. Select the diet for weight reduction: To prevent nutrient deficiencies when the patient is greater than 10% overweight, select a low-calorie weight reduction diet formulated with higher levels of protein, essential fatty acids, vitamins, and minerals to compensate for caloric restriction and possible decreased bioavailability of nutrients. Account for and incorporate treats or a list and amounts of "acceptable" foods to increase owner compliance (aim for no more than 5% of total diet). Calculate daily volume of food and treats to be fed; divide into two or more meals to decrease begging.
6. Implement exercise if patient can tolerate: Exercise can be delayed until some weight loss is achieved.
7. Reassess: Every 2 weeks until weight loss trend is established.If the animal fails to lose weight within 4 weeks, reduce intake further by 10% to 15%. Recheck monthly once weight loss trend is established.
8. Follow-up after reaching target weight: Select type and quantity of maintenance diet. Follow up every 3 to 6 months.
Take-Home Messages • Obese animals have increased risks for airway obstruction and respiratory distress. Although weight loss is not a "quick fix" and may be less appealing to owners than surgical or pharmacologic management of respiratory disease, it is often the most effective and lowest-risk therapy.• Improvement in respiratory function and clinical signs can be achieved in some obese patients with weight loss alone, which should be an important first stepin management of overweight patients with stable respiratory signs.