Rehabilitation After Stifle Joint Surgery
Denis J. Marcellin-Little, DEDV, Diplomate ACVS & ECVS, CCRP, North Carolina State University
Joanna Freeman, BSc PT, BSc Kine, CSCS, Animal Rehabilitation and Wellness Hospital, Raleigh, North Carolina
Overview
Surgery of the stifle joint is the most common orthopedic procedure done in the teaching hospital at North Carolina State University. Stabilization of CCL ruptures and medial and lateral patellar luxations are the most common stifle joint surgeries; others include correction of femoral, tibial, or patellar fractures involving the stifle joint, particularly Salter II fractures of the distal portion of the femur; correction of traumatic stifle luxations; and removal of osteochondral flaps in dogs with osteochondritis dissecans. Immobilization after surgery has clear detrimental effects in humans and in dogs; however, rehabilitation after stifle joint surgery, particularly after reconstruction of the anterior cruciate ligament, has definite benefits.1,2 Immediate postoperative rehabilitation includes passive range-of-motion exercise, ice application, stretching, and weight-shifting exercises; later rehabilitation primarily comprises protected strengthening exercises.
Rehabilitation is particularly important in patients facing permanent complications or in those with severe disease, including patients predisposed to permanent loss of joint motion because of age, trauma severity, repeated surgeries, long-term joint immobilization, or limb disuse. Patients with limited mobility due to size, age, body condition, fitness level, or comorbid conditions are also important candidates for rehabilitation.
The patient should perceive rehabilitation as a positive experience. A quiet, comfortable environment; positive reinforcement; and adapting the rehabilitation protocol to the patient's personality help achieve this goal. A miniature poodle that has had patellar surgery may be amenable to manual therapy but may be reluctant to perform therapeutic exercises.
A working Belgian shepherd may be less amenable to manual therapy but may perform well during therapeutic exercise sessions.
Most patients undergo rehabilitation without sedation. This allows the therapist to more objectively assess the pain management protocol as well as the joint. With proper pain management, patients tolerate gentle manipulation of the joint throughout the early postoperative period. Our conventional perioperative pain management protocol includes preemptive injection of an NSAID, epidural injection of an opiate and local anesthetic, and joint block with a local anesthetic; perioperative opiate administration; and early postoperative administration of an opiate. The postsurgical pain management protocol is administration of an NSAID and opiate analogue (tramadol hydrochloride) for 2 weeks. Pain is assessed at regular intervals and managed aggressively. Implementing a comprehensive pain management protocol is critically important to develop a positive relationship with the patient early and to sustain this relationship throughout therapy.
Step-by-Step: Early Postoperative Rehabilitation
The main goals of early rehabilitation are to control pain; maintain joint motion; eliminate edema; allow early, protected limb use; maintain proper posture; and decrease potential complications, including failure of fixation and infection.
What You Will Need
Simple tools may be used to assess joint angles, spinal reflexes, and limb circumference, respectively: (from left to right) a 15-cm transparent plastic goniometer, rubber-headed hammer, hemostatic forceps, and calibrated tape measure. An exercise ball is helpful for performing limb extension.

Step 1
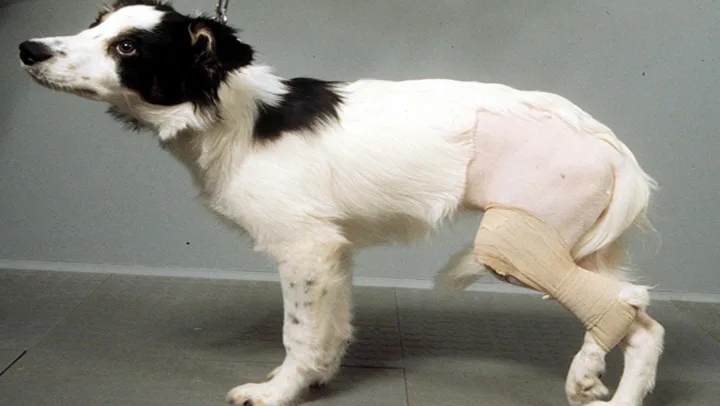
We usually do not bandage limbs after stifle joint surgery to avoid the negative effects of immobilization and to facilitate early rehabilitation. In trauma patients with significant edema, a soft, padded bandage may be placed on the limb to provide gentle compression for 1 to 2 days after injury or surgery. A flexion bandage (above) may be used in the immediate postoperative period, when weight-bearing is contraindicated. Early massage, cryotherapy, and range-of-motion exercises are performed with the bandage in place.
Procedure Pearl
Cryotherapy has few side effects. It is contraindicated in hypothermic patients and is used cautiously in miniature breeds.

Step 2
Rehabilitation starts immediately after surgery with cryotherapy on the operated area. The packs (inset) are frozen, double-lined plastic bags filled with two parts water and one part isopropyl alcohol. The pack is usually placed on the operated area or wrapped around it 1 to 12 hours after surgery for 10 to 20 minutes and repeated two to four times daily.3 Cold is a local vasoconstrictor-it decreases or inhibits bleeding; decreases local edema; reduces the metabolic rate, thereby reducing the production and release of inflammatory mediators; and inhibits collagenase. Cryotherapy has few side effects. It is contraindicated in hypothermic patients and is used cautiously in miniature breeds.

Step 3
Passive range-of-motion exercises are initiated 1 to 12 hours after surgery. The joint is gently flexed and extended 15 to 20 times, two to five times per day. These exercises decrease pain and edema and promote joint fluid motion in the operated stifle joint. Gentle massage is also used to decrease pain, edema, and muscle spasms. In patients with severe tissue trauma or a lower pain threshold, passive range-of-motion exercises are done more cautiously.

Step 4
Stretching is implemented once the acute postoperative pain subsides, generally after 2 to 3 days. In most patients, the focus is placed on regaining stifle joint extension. This is particularly relevant after extracapsular stabilization of CCL-deficient stifle joints because the prosthetic line tends to limit stifle extension. The anticipated gain in extension during the early rehabilitation period is 5 to 10 degrees per week. In some patients, maintaining or regaining flexion is particularly important. This is relevant in puppies since they are predisposed to losing motion in the stifle joint after surgery involving the pelvic limb. (The bars in A and B represent the long axes of the femur and tibia.) It is therefore critically important to perform range-of-motion and stretching exercises of the stifle joint in these patients. An exercise ball is often used for stretching exercises. Once the dog is in place on the exercise ball, the therapist places the leg in natural stance and slowly rolls the ball forward to provide a gentle stretch in extension (C). The ball may also be rolled from side to side to create a protected weight-shifting exercise.
Procedure Pearl
The anticipated gain in extension during the early rehabilitation period is 5 to 10 degrees per week.

A
Step 5
Weight-shifting exercises are also started 2 to 3 days after surgery, as soon as the patient begins to bear some weight on the operated limb. These exercises are aimed at increasing early limb use, which may limit muscle atrophy and the tendency to shift weight toward the opposite pelvic limb and forelimbs. The exercises are performed with the patient standing on the floor or on an exercise ball (see Figure 4C, above). A static weight-shifting exercise (left) is done by gently pushing on the hip region of a dog, leading it to shift weight from side to side.

Step 6
In the early postoperative period, on a daily basis, the owner assesses edema, comfort during manipulation, and limb use. The therapist and veterinarian overseeing the therapy assess stability of the surgical repair, joint effusion and crepitus, pain-free maximum range of motion (A and B), and potential changes in muscle mass. This assessment requires such tools as a goniometer, calibrated tape measure,4 rubber-headed hammer, and hemostatic forceps. In C, a calibrated tape measure is being used to measure the thigh of a dog with severe osteoarthritis of the stifle joint. To maximize repeatability, the measurement is made with the stifle joint in extension, at a point 70% along the femur.
Procedure Pearl
The patient should be exercised without creating excess fatigue or loss of limb function. Mild fatigue should be recognized and adequate rest periods provided.

A & B
Step 7
In the weeks after surgery, stretching may be continued if the range of motion is still limited. Heat, which may be delivered using a moist heat pack or therapeutic ultrasound, is placed on the tissue before and during stretching to enhance the benefits of stretching. The therapeutic temperature range for heated tissue is 43° C to 45° C (109.4° F to 113° F). In this case, therapeutic ultrasound (5 cm2 head, 1MHz, continuous) is being used to heat the quadriceps femoris muscle before stretching the stifle.
Procedure Pearl
Common exercises done in dogs to regain functional strength include walking, transitions from sitting to standing and vice versa, stair climbing, walking on an incline, and walking in water.

Step 8
Functional strength is required for independent living. Regaining functional strength is the main rehabilitation goal after the immediate postoperative period, focusing on strengthening the hamstrings, gluteals, and quadriceps. This is generally achieved through exercises but may also be done with neuromuscular electrical stimulation (A) if exercise is not possible. The early strengthening period should include low-intensity therapeutic exercises of short duration-for example, more repetitions with limited weight placed on the affected limb. Common exercises done in dogs to regain functional strength include walking, transitions from sitting to standing and vice versa, stair climbing, walking on an incline, and walking in water. The dog in B is exercising on an underwater treadmill at 1 m/s (2.3 mph) with water up to his flank fold.

A
General Guidelines & Goals
Fatigue, like pain, is an important consideration in the early postoperative stage. The patient should be exercised without creating excess fatigue or loss of limb function. Mild fatigue should be recognized and adequate rest periods provided. Exercises should be done in an area with good traction that is free of obstacles. In the beginning, the exercise session should last only a few minutes, ideally in three to five sessions per day, with a gradual increase in intensity and duration. Once functional strength is achieved, more challenging exercises may be introduced. The goals for each patient differ based on age, breed, purpose in life, and fitness level. More challenging exercises include hill walks of varying grades, underwater treadmill walking with jets for resistance and incline, jumping activities (plyometrics), exercising on different surfaces (i.e., pine straw, gravel, grass, sand), using a trampoline, and balance-board activities. The intensity (i.e., adding a weight vest), speed, and duration of these exercises should be increased as needed to challenge the patient during reconditioning.
Long-term functional assessment is important and should be done every few months. This includes reassessing range of motion, muscle mass via girth measurements, quantity and quality of limb use, presence or absence of swelling or effusion, presence or absence of crepitus, efficiency and ease of functional activities, gait analysis, and testing for instability or anomalies.