Reflux Esophagitis
A 2-year-old neutered male Siamese cat is presented for regurgitation.
History. The owner reports regurgitation of 1 week in duration. She describes the episodes, which occur immediately after eating, as passive in that they are not associated with retching. The cat seems distressed after eating, the food is expelled immediately after swallowing, and the cat often tries to ingest the food a second time. The patient is reported to be better able to ingest liquids or water. It had also been treated 3 weeks earlier with doxycycline tablets for an upper respiratory tract infection. The cat presented for the current complaint two weeks after discontinuation of the medication.
Examination. The physical examination is unremarkable.
Laboratory Results. The results of a CBC, biochemical profile, and urinalysis are normal.

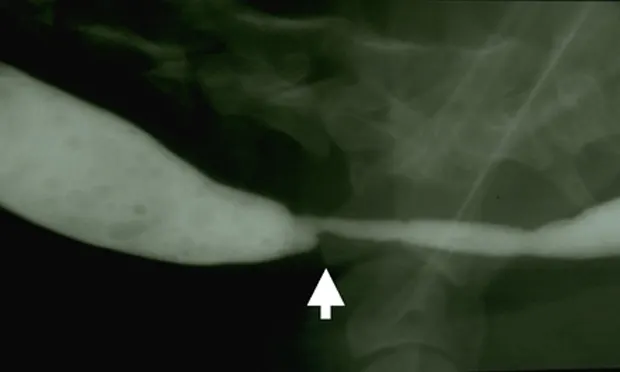
Radiographs. Thoracic and abdominal radiographs are considered normal. A liquid barium contrast study is performed, and no obvious abnormalities are detected. Because the regurgitation episodes are worse when associated with ingestion of solid food and less with liquids, a barium-food esophagram should be performed. Figure 1 is a barium-food esophagram that shows a narrowing of the esophagus at the thoracic inlet with esophageal dilatation cranial to the defect. Endoscopy might be performed rather than the barium-food esophagram if it is available in the practice.
Figure 1. A barium-food mixture esophagram showing dilatation of the cervical esophagus with a luminal narrowing at the thoracic inlet (arrow)
ASK YOURSELF ...Based on the clinical description and radiographic findings, what is the optimal diagnostic or therapeutic plan for this case?
A. Perform surgical resection of the esophageal defect.B. Perform endoscopy and balloon dilatation.C. Treat the cat with metoclopramide and famotidine.D. Recommend feeding a semiliquid hypoallergenic diet.E. A and B
Correct Answer: BPerform endoscopy and balloon dilatation.
The most likely cause of this abnormality is an intramural esophageal stricture. Unlikely causes for esophageal narrowing include extrinsic extraesophageal compression from neoplasia or inflammation, vascular ring anomaly, presence of an esophageal foreign body, or esophageal neoplasia. Endoscopy was done to delineate the obstruction and to perform therapeutic esophageal dilatation. Figure 2 shows the esophageal narrowing at the thoracic inlet. Figure 3 shows the esophagus following a balloon dilatation procedure.

Figure 2. Endoscopic view showing a benign focal esophageal stricture secondary to a doxycycline tablet in a cat
Benign intramural esophageal strictures usually occur after submucosal ulceration with subsequent fibrosis. Animals with strictures generally regurgitate solid food but can usually hold down liquids unless the stricture is severe. In several reviews of dogs and cats with esophageal strictures, anesthesia-related gastric acid reflux was reported to be the most common cause. Animals having gastric reflux-associated strictures generally present several weeks after being anesthetized, and the strictures are most often located in the distal esophagus. Other causes of esophageal stricture include esophageal foreign bodies, pill-associated stricture formation, esophageal trauma, and trauma secondary to esophageal tube placement.

Figure 3. The esophageal stricture after dilatation to 16 mm diameter
Doxycycline is reported to be one of the most common antibiotics associated with secondary esophagitis in humans. Pill-associated esophageal stricture secondary to doxycycline tablet administration has also been reported in cats. In a recent case series, the most common location for feline doxycycline-induced esophageal stricture was the proximal esophagus. It is believed that pill-associated strictures occurred due to the prolonged direct irritant effect of the doxycycline on the esophageal mucosa. Studies in normal cats have shown delayed passage of tablets through the esophagus when given as a "dry" swallow without water, lubricants, or food. The pills most commonly lodge in the cervical esophagus.

Treatment Plan. Feed a liquid diet or attempt to dilate the stricture. Surgical resection is considered to be less successful. Several dilatation instruments have been described, but dilatation with a balloon seems to be the safest and most successful method. Balloons of increasing diameter are inserted into the lumen and then inflated under pressure to open the lumen to the desired diameter. In this case, the stricture was dilated to 16 mm in diameter over a course of three sessions at weekly intervals. Some authors recommend systemic or intralesional injections of steroids to reduce inflammation and stricture contraction. This cat was also treated with intralesional injections of triamcinolone in the stricture site using an endoscopic injection needle. It made an uneventful recovery and now consumes canned food without problems.
Take-Home Messages
Strictures can be delineated radiographically using a barium-food mixture. If endoscopy is available, it is the definitive means of diagnosing esophageal stricture.
Inflammatory strictures of the esophagus are best treated with endoscopic balloon dilatation.
Doxycycline tablets, anesthesia-associated gastric acid reflux, and foreign bodies are the most common causes of stricture formation.
Dilatation of esophageal strictures often requires referral to a specialist.
TX at a glance...
Feed a liquid diet.
OR
Attempt balloon dilatation. Insert and inflate balloons of increasing diameter over a course of weekly sessions.
Consider intralesional steroid injections.