Recurrent Hematuria in a Dog
Erin Galemore, DVM, Cummings School of Veterinary Medicine at Tufts University
Mary Anna Labato, DVM, DACVIM (SAIM), Cummings School of Veterinary Medicine at Tufts University

Sadie, a 5-year-old spayed terrier crossbreed, was presented with recurrent, intermittent hematuria of 2 years duration.
History
Over 2 years, Sadie had 5 to 6 episodes of gross hematuria lasting for 3 to 5 days each; no other clinical signs were apparent during the episodes. CBC and serum chemistry profile measured at a later episode were within normal limits. Abdominal radiographs during the same episode appeared normal; cystic calculi were not observed. Urinalysis during 2 of the hematuria episodes showed concentrated urine (USG 1.05), pH 8.0, hematuria (10-50 RBCs/hpf, 2-3 WBCs/hpf), proteinuria (1-2+ on dipstick), and struvite crystalluria. No pollakiuria or stranguria was noted. No bacteria were seen on sediment examination. Culture and susceptibility testing results obtained during 2 episodes were negative.
During the 2-year period, Sadie was treated empirically with multiple rounds of antibiotics (ie, amoxicillin 22 mg/kg q12h, amoxicillinclavulanic acid 13.75 mg/kg q12h, marbofloxacin 5.5 mg/kg q24h) for suspected UTI. She was up-to-date on vaccinations and received monthly heartworm, tick, and flea preventive.
Physical Examination
On presentation, Sadie was bright, alert, and responsive. Physical examination and vital signs (ie, heart rate, respiratory rate, temperature) were within normal limits. No additional abnormalities were identified.
Diagnostic Results
Abdominal ultrasound showed a mildly thickened cranioventral urinary bladder wall with a 6-mm irregular, polypoid, inhomogeneous mass extending into the lumen (Figure 1). No other abnormalities were identified in the abdomen. Cystoscopy revealed an irregular mass on the cranioventral wall with an area of ulceration and a fibrous tag protruding into the lumen (Figure 2). The remainder of the bladder appeared friable. Aerobic and Mycoplasma spp cultures of the bladder wall were negative. Histopathologic examination of biopsies showed mild lymphocytic cystitis.
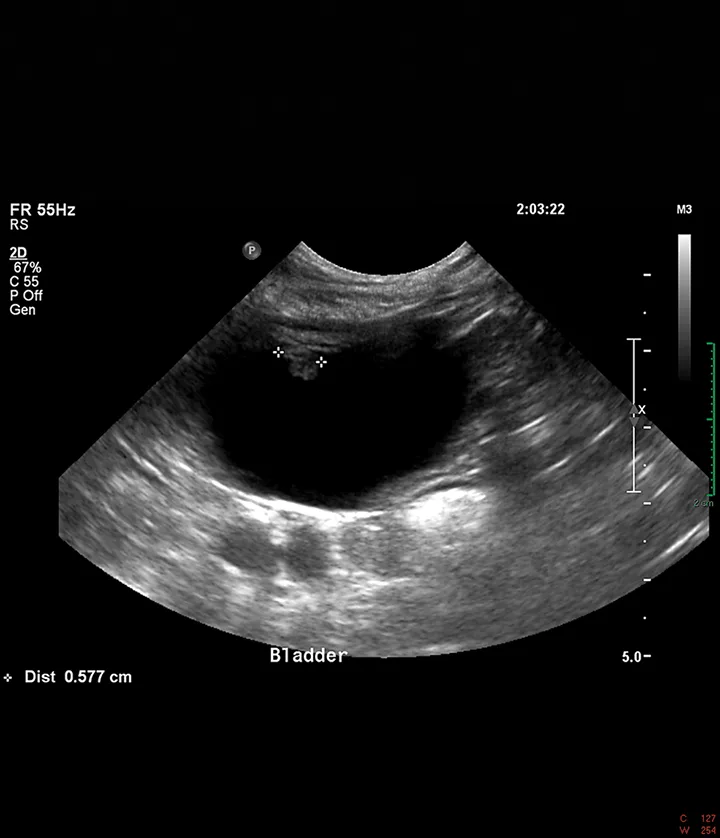
Ultrasound image of a 6-mm polypoid mass extending into the lumen from the cranioventral bladder wall
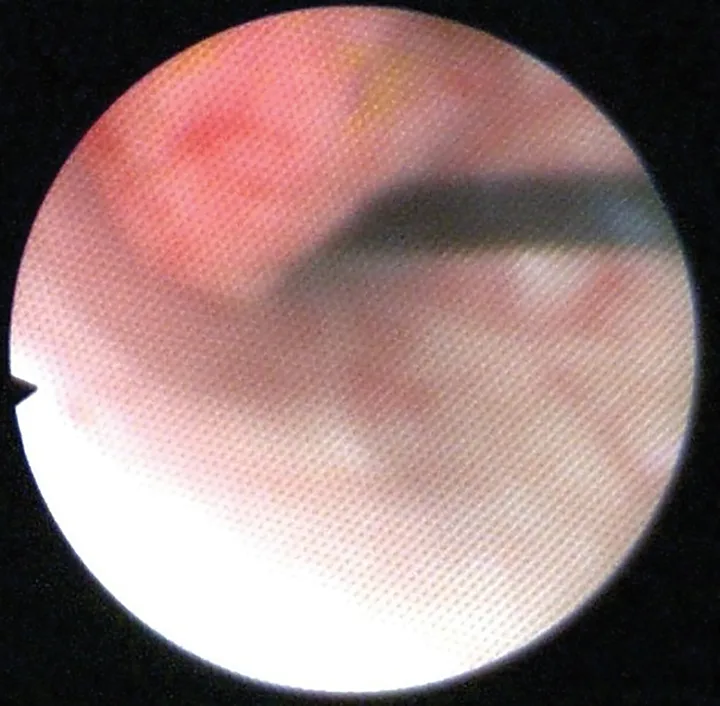
Cystoscopic image of an ulcerated polypoid mass extending into the bladder lumen
Diagnosis
Polypoid cystitis
Treatment
Sadie received a 5-day course of oral enrofloxacin at 10 mg/kg/day while tissue and urine culture and susceptibility results were pending. She was also prescribed oral meloxicam at 0.1 mg/kg/day for 30 days to treat suspected polypoid cystitis.
Outcome
After treatment with meloxicam for 30 days, follow-up abdominal ultrasounds showed complete resolution of the bladder mass. Despite one episode of hematuria, which responded to meloxicam, Sadie had no additional clinical disease 3 years postdiagnosis.
Overview
Polypoid cystitis is an uncommon disease in dogs characterized by proliferation of the bladder mucosa, which can cause thickening of the bladder wall, papillary-like projections from the mucosal surface, and polyps that extend into the bladder lumen.1,2 These lesions are most commonly seen on the cranioventral bladder wall.1-3 The main differential diagnosis for masses in the bladder is malignant neoplasia (eg, transitional cell carcinoma).1,2 Polyps are often ulcerated, which can lead to hematuria.1,4 Clinical signs of polypoid cystitis include hematuria, stranguria, and pollakiuria. This disease is seen more commonly in female dogs.1 The most common presenting complaint for these patients is hematuria and/or recurrent UTI.1,2
Pathophysiology
The cause of polypoid cystitis in dogs remains unclear; however, chronic inflammation of the bladder mucosa is thought to cause this proliferative tissue.1,2,4,5 Chronic UTI and cystic calculi also have been associated with development of polypoid cystitis.1,2,4,5 Polypoid cystitis is common in humans and is usually a complication of chronic urethral catheterization; however, this association has not been documented in canine patients.1,6,7 Catheter removal can lead to regression of bladder lesions in most human patients with catheter-associated polypoid cystitis.8 Removal of the inciting cause and control of inflammation have been anecdotally suggested as medical management for polypoid cystitis in dogs; however, no reports in the literature substantiate this recommendation.
Polyps could represent a preneoplastic condition; however, this has not been recognized in the literature. In a 2003 case series on polypoid cystitis, one canine patient was reported to have recurrent UTI, cystolithiasis, and polypoid cystitis over the course of 8 years; this patient was subsequently diagnosed with transitional cell carcinoma 8 years after the initial diagnosis of polypoid cystitis.1 To the authors knowledge, no other reports have shown malignant transformation of polypoid cystitis to transitional cell carcinoma in dogs.
Diagnosis
Diagnosis of polypoid cystitis is based on lesion location and histopathologic examination. Polyps are most commonly located on the cranioventral bladder wall, whereas transitional cell carcinomas are most commonly located in the trigone of the bladder.1-3,9 A single mass or multiple masses may be present.1,3,7 Definitive diagnosis requires histopathologic examination. Biopsy samples can be obtained via cystoscopic or surgical approach. Cystoscopically obtained biopsies are small and often contain crush artifact, which can impede diagnosis.1 Surgical biopsies are required for definitive diagnosis for cases in which cystoscopic samples are suggestive of polypoid cystitis.1 Histologic lesions include mucosal ulceration, solid downgrowths of epithelium, stromal edema, cyst-like intraepithelial structures, chronic inflammation, and evidence of chronic hemorrhage.1,5,7 The lack of invasion into the muscularis layer and low mitotic activity of polypoid lesions help differentiate this disease from transitional cell carcinoma.1,5,7 The severity and character of inflammation in these lesions are highly variable with lymphoplasmacytic, neutrophilic, histiocytic, and eosinophilic infiltrates reported in the literature.1,4,5
Treatment
Treatment of polypoid cystitis is focused on removing the inciting source of inflammation and reducing inflammation, as well as potential surgical excision of the polyp(s).1,2,4,5 Treatment should involve targeted antimicrobial therapy based on urine and/or bladder wall culture and susceptibility testing to eliminate infection. Extended courses of antimicrobial therapy (eg, 4-6 weeks) may be required to eliminate infection.1 Cystoliths should be removed, as stones can precipitate inflammation in the bladder and act as a nidus for infection.1,2 NSAIDs can reduce inflammation in the bladder. In severe cases, surgical excision of the polyps and/or partial cystectomy is required to resolve clinical signs.1,4,5 All reported cases of canine polypoid cystitis in the literature were treated surgically to remove the lesions and cystoliths, if present, with adjunctive treatment for infection when indicated.1,4,5,10 Control of infection and urolithiasis is paramount to prevent recurrence of polypoid cystitis.1,10 Dogs with recurrent UTI and cystolithiasis are at risk for recurrence of polypoid cystitis.1
Long-term follow-up should consist of frequent monitoring for UTI via urine culture and monitoring for polyp recurrence via contrast radiography or ultrasonography. Information about prognosis and long-term outcome in the literature is sparse, but surgical removal of these lesions has been associated with good outcome and resolution of clinical signs and visible lesions; however, recurrence is possible.1,4,5,10