Ovariohysterectomy vs Ovariectomy
Elective sterilization of female dogs and cats through gonadectomy, one of the most common surgical procedures in small animal practice,1 has many purposes, including eliminating behavioral changes associated with hormonal cycles, controlling canine and feline populations, and preventing diseases favored by having an intact status (eg, mammary tumors, cystic endometrial hyperplasia or pyometra).
Described techniques include removal of the ovaries through a ventral midline, flank, or minimally invasive approach. In some countries, including the U.S., the standard procedure involves concurrent surgical removal of the uterus (ovariohysterectomy [OVH]); some common American textbooks still lack discussion of ovariectomy (OVE).2-5 Conversely, for decades in many European countries, OVE has been the standard procedure for spaying animals without uterine disease.
Uterine Disease
It is assumed OVH can be preferred over OVE because it would better prevent uterine disease; however, except for tumors, uterine diseases do not occur in the absence of endogenous or exogenous hormonal exposure.6 No indications exist for the administration of exogenous progestagens,7 and, although endogenous progesterone is also secreted by the adrenal glands,8 it is not produced in clinically relevant amounts in the absence of ovaries. Therefore, in the absence of supplemented exogenous progesterone, animals that undergo OVE with a healthy uterus are unlikely to develop such uterine diseases as cystic endometrial hyperplasia or pyometra later in life.
In one study,6 owners of bitches that had elective OVE (n = 69) or OVH (n = 66) 8 to 11 years earlier completed a questionnaire; none of the bitches appeared to have developed endometritis or ovarian remnant syndrome (ORS), and there were no differences between the procedures with regard to incidence of other potential complications (eg, urinary incontinence). In another study in which OVE was performed on 72 bitches, none developed pyometra over the following 6 to 10 years.9
Pyometra or stump pyometra can occur with ORS, after either OVE or OVH, and results from failure to remove all ovarian tissue at surgery; ORS is almost exclusively a consequence of improper surgical technique.10 Most reported cases of ORS have been associated with OVH,9 but this finding may reflect the more common performance of OVH as compared with OVE in the countries from which these reports originated. At first glance, ORS might be considered more likely with OVE, as two tissue sections are made close to the ovary in OVE, while only the ovarian pedicle is severed close to the ovary with OVH.9 However, in OVE the ligature and section situated on or near the proper ligament of the ovary are the easiest to perform, making it simple to be far enough away from the ovary (especially as the tip of the uterine horn can be excised with the ovary).
The more cranially located incision used for OVE may allow better visualization of the ovary and ovarian pedicle than is possible with OVH, thereby decreasing risk for ORS.9,10 Regardless of whether OVE or OVH is performed, ORS can be prevented before closing the abdomen by systematically inspecting the excised ovary to verify that it has been entirely removed. In cats, this is done by direct inspection, as the ovary is generally directly visible, and in dogs by opening the ovarian bursa through complete extension of its medial opening. Failure to verify removal of excised ovaries may be considered malpractice.
Uterine neoplasia can develop after OVE; however, uterine tumors are reportedly rare (0.03%) and are benign in 85% to 90% of cases.11 Therefore, the overall risk for developing a malignant uterine tumor after OVE has been estimated to be 0.003%.9 This risk has to be balanced against the disadvantages of OVH compared with OVE in terms of surgical time, additional trauma, and potential complications. Furthermore, the protection OVH provides against uterine tumors is not absolute, as variable amounts of the uterine body are often left in place.
Complications & Consequences
From a theoretical standpoint, OVE is expected to result in less surgical trauma, as the required incisions are smaller and fewer anatomic structures are involved.
One randomized, prospective trial in 40 dogs found OVH to be associated with significantly longer cutaneous and fascial incisions as compared with OVE, without any difference in total surgical time, postoperative pain scores, and short-term complications (eg, blood loss, erythema, swelling, wound discharge, dehiscence).11 However, this study was conducted in an academic environment, and the operations were done by a board-certified surgeon assisted by a veterinary student. Whether the same conclusions would be reached from a similar study conducted in general practice is unknown. Another study involving only a few patients found that OVE was associated with shorter incision lengths, shorter anesthetic and surgical times, lower postoperative pain scores, and less surgical stress response than was OVH.12
A review of the theoretical and reported risks of OVE and OVH showed that more complications should be expected with OVH.11 Potential complications associated with ligation of the ovarian pedicle and ORS were considered similar for both procedures. Specific risks associated with ligation of the proper ovarian ligament were assumed minimal, but specific risks inherent to removal of the uterus, such as hemorrhage from the broad ligament or uterine vessels, ligation of the caudal intraperitoneal portion of the ureter(s), and postoperative vaginal bleeding, were considered significant.11
Well-known, long-term benefits of spaying (eg, prevention of mammary tumors or nonneoplastic uterine disease) and its long-term complications (eg, urinary incontinence, weight gain) are expected to be similar for OVE and OVH, as both are hormone dependent. Similarly, both procedures equally eliminate any ovarian interference with systemic diseases (eg, diabetes mellitus, epilepsy).13,14
Minimally Invasive Spay Procedures
Minimally invasive surgery is becoming increasingly common, and elective spaying is one of the most common indications for laparoscopy. Both OVE and OVH can be performed laparoscopically, although minimally invasive OVH is most commonly performed as a laparoscopic-assisted procedure to facilitate ligation and section of the uterine body or cervix.10 Laparoscopic OVE is technically easier and quicker than laparoscopic OVH and usually reduces the number of required incisions by at least one.15 Development of minimally invasive spay procedures may likely be the single best worldwide promoter of OVE.
In My Opinion…
When OVE and OVH are properly performed, with appropriate and sufficient exposure, they are both safe procedures, although OVH may expose the patient to more complications. The disadvantages of routinely performing elective OVH rather than OVE lie in the approach in general practice rather than a significant difference in inherent risks.
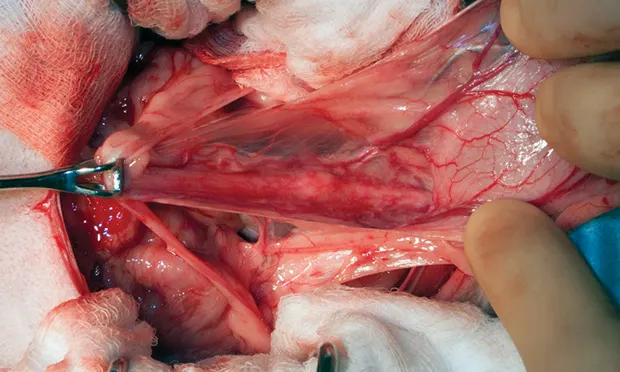
For various reasons, probably including time constraints, OVH is often performed through an as-small-as-possible abdominal incision, whether a ventral midline or flank approach is used, that is located to attempt to allow visualization of both the ovaries and the cervix but is optimal for neither; this can result in relatively poor exposure. Significant traction is required to reach the uterine body, and excessive traction on the uterus has been associated with rupture of uterine vessels and hemorrhage16 and is unnecessarily traumatic. Often, the cervix cannot be reached and identified when using a small incision approach; the uterus is, therefore, ligated and sectioned either without precise visual control, which exposes the patient to complications (Figure 1), or too cranially, leaving a significant portion or all of the uterine body (Figure 2). Such an incomplete resection is unlikely to cause problems but somewhat negates the putative advantages of OVH. This difficulty in reaching the cervix may be even greater with a flank approach,10,17 requiring considerable retraction of the abdominal wound, which may contribute to more postoperative pain than would a ventral midline approach.18
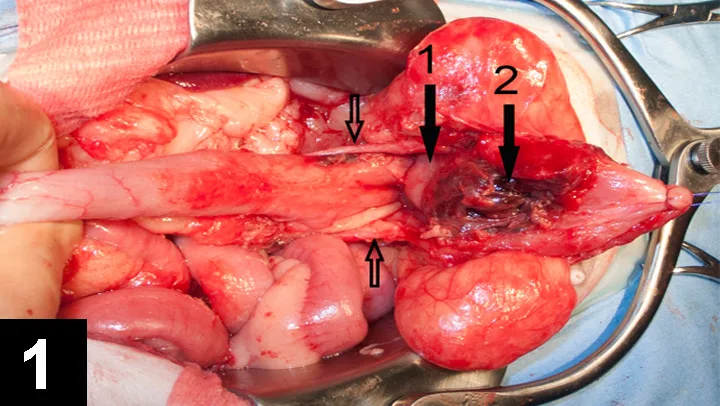
Partial bladder necrosis from vascular compromise after ovariohysterectomy (white arrow, uterine stump; yellow arrow, necrotic portion of the bladder; black arrows, ureters) in a dog
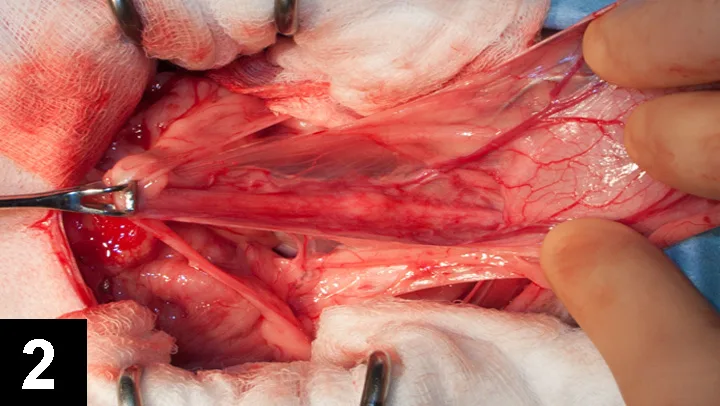
Intraoperative view of a uterine stump reveals that the cervix (yellow arrow) and most of the uterine body (white arrow) remain in place in this dog.
Veterinarians continue to seek rapid, safe spay options through small or minimally invasive approaches, and OVE is a reasonable choice to fulfill these criteria. OVE can provide the same health benefits as OVH, except for prevention of exceptional uterine neoplasia. Varying levels of evidence show that OVE requires smaller incisions, creates less surgical trauma, results in less pain, and carries a smaller risk for complications.9,11,12,19 Lastly, the elective resection of a healthy organ in the absence of a high risk of future disease may contradict the universally praised principles of a traumatic surgery.