This response is correct!
Oral Tumors
Sarah Boston, DVM, DVSc, DACVS, ACVS Founding Fellow of Surgical Oncology, ACVS Founding Fellow of Oral & Maxillofacial Surgery, VCA Canada, Newmarket, Ontario, Canada

Almost 100% of oral tumors in cats and 95% in dogs are malignant. Because of these high malignancy rates, it is critical that oral masses be detected and biopsied early in the disease course.
History & Clinical Signs
Dogs and cats with oral tumors may exhibit halitosis, ptyalism, bleeding from the oral cavity, facial asymmetry, and/or dysphagia. Patients may be presented for dental prophylaxis due to perceived or actual dental disease. A thorough, systematic oral examination should be performed during physical examination, dental prophylaxis, and procedures with general anesthesia, because this is when oral tumors are often discovered. Clinicians should be prepared to conduct a diagnostic investigation, such as incisional biopsy, during these procedures.
Physical Examination
Patients with oral tumors should undergo a thorough physical examination, including a digital rectal examination, to rule out other malignancies (eg, anal sac adenocarcinoma or transitional cell carcinoma that can metastasize to other bone sites such as the mandible).
Diagnostics
Staging tests may include dental radiography, 3-view thoracic radiography, and aspiration of the mandibular lymph nodes. A CT scan of the head and thorax is typically recommended for local and distant staging and surgical planning, especially for gingival tumors (Figure 1). For acanthomatous epulides, a CT scan of the thorax may not be necessary, as these tumors are locally aggressive but do not metastasize. Additional testing prior to surgery should include CBC, serum chemistry profile, urinalysis, and, in case blood transfusion becomes necessary, blood typing.
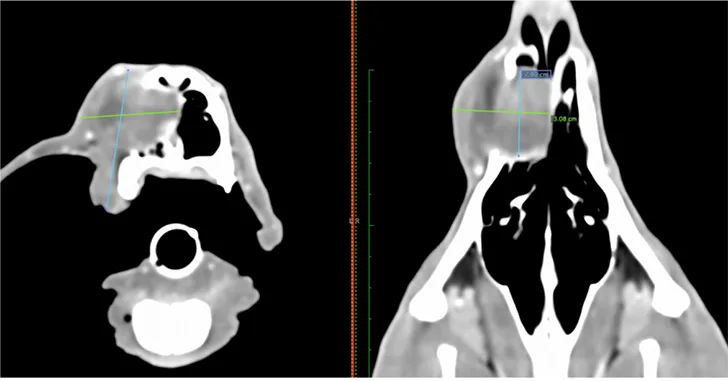
CT scan of a 1-year-old dog with a high-grade fibrosarcoma of the maxilla
Diagnosis
Definitive diagnosis is required once an oral tumor is identified. Common differential diagnoses for oral tumors in dogs include malignant melanoma, squamous cell carcinoma, fibrosarcoma, osteosarcoma, and acanthomatous epulis.1 In cats, squamous cell carcinoma, osteosarcoma, and fibrosarcoma should be considered. Although it is beneficial to ensure that the oral cavity is as clean as possible prior to surgical resection and/or radiation, some pet owners may prefer to know diagnostic and treatment options before proceeding; therefore, the pros and cons should be discussed with the owner before biopsy or dental prophylaxis is performed.
Definitive diagnosis is best achieved via histopathology (vs cytology), and incisional biopsy of the oral cavity is recommended. The biopsy tract should be removed with definitive resection, as it will likely be contaminated with tumor cells; this is especially important for tumors of the maxilla, as biopsy through overlying skin can complicate reconstruction techniques after maxillectomy. The oral mucosa can heal quickly and—in patients in which an oral mass has been marginally excised—the removal site may no longer be evident by the time histopathology results are received; this can lead to a suboptimal outcome when wide tumor resection or radiation treatment is planned. Thus, excisional biopsy is not recommended for oral masses. Shaving off the mass should be avoided. It is also recommended that digital photographs of the mass be taken while the patient is under anesthesia or sedated, especially if the patient is to be referred to a specialist.
In dogs, high-low fibrosarcomas are an extremely locally aggressive fibrosarcoma subtype that is biologically high-grade but appears to be low-grade on histopathology (Figure 2).2 A high-low fibrosarcoma has the potential to be misdiagnosed on incisional biopsy because the tissue can appear microscopically as a histologically bland or benign inflammatory lesion. A description of the mass and the presence of bone lysis on radiographs or CT images are critical to histopathologic interpretation. A pathologist should be consulted if the histopathologic diagnosis does not fit clinical characteristics.
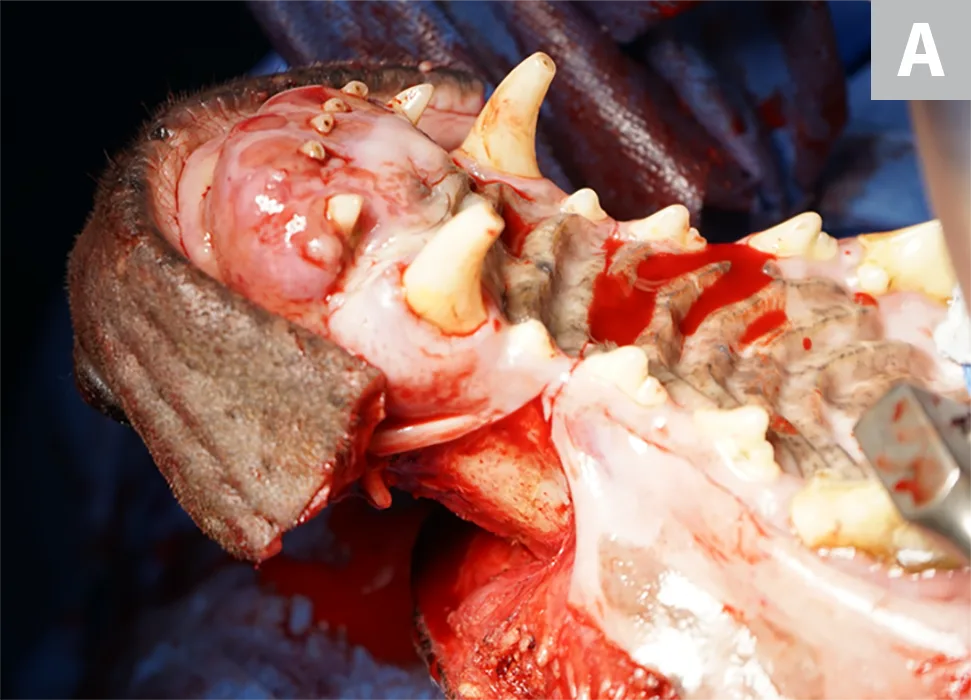
FIGURE 2A
A 9-year-old neutered male Doberman pinscher with a high-low fibrosarcoma of the maxilla (A). Wide margins and radical maxillectomy are required for complete resection and performed with an oscillating saw (B). Margins of excision were complete 2 weeks postoperatively (C), and he was eating well at home.
Additional Considerations
In cats, squamous cell carcinoma is the most common oral tumor, followed by osteosarcoma.1 Although the underlying cause of most oral tumors is poorly understood, eating canned tuna, wearing flea collars, and living with humans who smoke have been associated with potential oral tumor risk in cats.3,4 Oral papillomavirus may be associated with some cases of squamous cell carcinoma in dogs.5,6
Treatment & Management
In dogs and cats, malignant tumors of the oral cavity should generally be treated with wide excision (ie, cheilectomy, glossectomy, mandibulectomy, or maxillectomy, depending on the tumor location) of the mass. Most malignant tumors of the gingiva invade the underlying bone to some degree, and the affected portion of the mandible or maxilla should be removed with a minimum margin of 1 cm; this is similar for lip and tongue tumors. In dogs, ≤70% to 80% of the tongue can be removed and still have the potential to return to function.7,8 Wide excision is not possible for tonsillar tumors, for which marginal excision is generally recommended. Elective lymph node dissection9 and/or sentinel lymph node mapping10 is recommended for surgical staging of disease.

FIGURE 3A
A 10-year-old spayed kelpie crossbreed with a high-low fibrosarcoma of the right caudal maxilla (A). The bipedicle flap created through a combined-approach maxillectomy to allow access to the maxilla dorsally and ventrally for en bloc resection can be seen (B); this flap should be preserved during incisional biopsy. After maxillectomy, the mucosa is elevated from the bipedicle flap and used to reconstruct the defect in the mouth (C and D). The patient appeared to do well 1 day (E) and 3 months (F) postoperatively.
Mandibulectomy & Maxillectomy
Mandibulectomy and maxillectomy (Figure 3) are the most common surgical procedures for gingival tumors in dogs and cats. For specimens, margins should be inked for histopathology and evaluation. Potential complications include hemorrhage, infection, dehiscence, incomplete excisional margins, mandibular drift, malocclusion, anorexia, dysphagia, and mass recurrence. Seroma formation is common at the lymph node dissection site.
Although novel techniques to restore the mandible are becoming available and involve either a 3D-printed implant11 or plate reconstruction and bone morphogenic protein, they are not commonly used.12 Clinicians should be prepared for blood transfusion. After maxillectomy or mandibulectomy, most dogs will eat within 24 to 48 hours postoperation and do not require placement of a feeding tube; however, feeding tubes should be considered for radical resections, especially radical maxillectomy. Although it is generally believed that cats do not do well after maxillectomy or mandibulectomy because they will not eat postoperatively, this has not been the author’s experience. There is potential for success with these procedures in cats. Feeding tubes are critical for cats, because they may not readily eat after surgery, and hepatic lipidosis is possible after even short periods of anorexia. A recent study of 8 cats that underwent radical mandibulectomy found that 6 cats ate on their own 3 days to 1 month postoperatively and had an estimated mean survival time of 712 days.13 A feeding tube is recommended in both cats and dogs after glossectomy.
In dogs and cats, multimodal pain control (primarily with a combination of opioids, NSAIDs, and local anesthesia) is recommended. Patients should be maintained on IV fluids and monitored for pain, hydration status, and evidence of ongoing hemorrhage. A patient’s ability to eat postoperatively may depend on the amount of tissue resected, amount of postoperative swelling, degree of pain control, and patient’s willingness to eat; canned food of different consistencies should be offered. Patients should wear an Elizabethan collar postoperatively.
Adjunctive Therapy
Recommendations for adjunctive therapy in dogs depend on tumor type and stage, as well as margin evaluation. Follow-up radiation therapy should be considered if clean histologic margins are not achieved. Oral melanoma is responsive to hypofractionated radiation, which involves weekly radiation therapy for 4 weeks. This protocol has minimal adverse effects and should be considered in patients deemed nonsurgical or in cases in which the owner chooses not to pursue surgery. Melanoma can also generally be treated with the melanoma vaccine rather than with chemotherapy.14,15 Systemic chemotherapy can be considered in dogs with osteosarcoma or patients with squamous cell carcinoma or fibrosarcoma in which there is evidence of lymph node involvement, a high-grade tumor, or high mitotic count.
Prognosis & Prevention
Prognosis with surgical treatment varies based on tumor type. Long-term survival is possible for patients with squamous cell carcinoma and with some sarcomas that have no evidence of metastatic disease, low metastatic potential based on histopathologic features, and complete surgical margins. The median survival time for patients with oral melanoma treated with surgery is 1 year.16
Although it is generally not possible to prevent oral tumors, it is recommended that pets not be exposed to household smoke. Regular physical examinations including the oral cavity and dental prophylaxis may help with early diagnosis, generally resulting in a better outcome and decreased need for surgery.
Clinical Follow-Up & Monitoring
Follow-up depends on the patient and disease, but oral examination, lymph node palpation, and 3-view thoracic radiography are recommended every 3 months for 1 year postoperatively. The owner should perform regular oral examinations at home and schedule a re-evaluation if there are any signs of recurrence or physical changes (eg, redness, swelling, mass development) in the area.