Oral Trauma: Caught Between Two Jaws

A 4-year-old, neutered male domestic shorthair presented with severe facial trauma.
History. The owner reported that the family dog attacked the cat when it approached the dog's food bowl. The owner brought the cat to her regular veterinarian for initial treatment. A CBC and chemistry profile were done. An IV catheter and esophagostomy tube were placed. Fluid therapy, nutritional support, antibiotics, and pain management were initiated. The cat was transferred the next day to the Animal Dental Center for oral surgery.
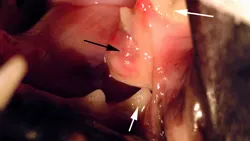
Examination. On presentation, the cat could not close its lower jaw. The mandible had lateralized to the animal's left side. A prominent, open symphyseal fracture covered with granulation tissue (Figure A) was visible, and the cat resisted physical manipulation. The

animal was anesthetized for further evaluation of the oral cavity. An open caudal fracture of the left mandibular ramus was visible between the 4th premolar and the 1st molar (Figure B; white arrows). The mandibular artery had been lacerated, and an organized fibrin clot was present (black arrow). An intraoral occlusal view radiograph was taken of the symphysis, and an extraoral lateral radiograph was taken of the TMJ and horizontal ramus of both right and left sides. A 1-cm separation of the symphysis was visible on the films, but no rostral mandibular fractures were present (Figure C). The left lateral film showed a caudal ramus fracture between the 4th premolar and the 1st molar (Figure D). There was no evidence of roots in the fracture site. This film also showed a left craniodorsal TMJ luxation (black arrows) and a left caudal ramus fracture between the 4th premolar and the 1st molar (white arrows).
ASK YOURSELF...Based on the animal's clinical presentation and the radiographic findings, what is the optimal therapeutic approach for this multilocalized trauma?
A. Use an intramedullary pin in the mandibular canal and a bone screw for symphyseal stabilization.
B. Transverse pin the symphysis, and place a figure 8 cerclage wire around the canine teeth. Use a 4-hole bone plate on the horizontal ramus. The TMJ will align itself.
C. Perform hemimandibulectomy. Due to the mandibular artery laceration, attempting fracture stabilization would be associated with a guarded prognosis.
D. Establish dental occlusion by open TMJ reduction. Reduce the symphysis and caudal mandibular fractures, and provide fixation with interdental splints and interosseous wire.
E. Perform mandibular condylectomy to prevent repetitive TMJ luxations, and temporarily splint the canines to allow the ramus fracture to heal by self-alignment.
Correct Answer: DEstablish dental occlusion by open TMJ reduction. Reduce the symphysis and caudal mandibular fractures, and provide fixation with interdental splints and intraosseous wire.
The TMJ is a hinge joint. The condyle is maintained in position by the joint capsule and the strong lateral ligament. Craniodorsal luxation is more often seen with mandibular trauma. The animal is usually unable to close the jaw, and when craniodorsal luxation is the sole trauma, it presents with mandibular lateralization to the contralateral side. In this case, symphyseal fracture and ipsilateral caudal ramus fracture were also present; as a result, the mandible shifted to the ipsilateral side of the trauma. Open TMJ reduction was done because of the concurrent symphyseal and horizontal ramus fractures.
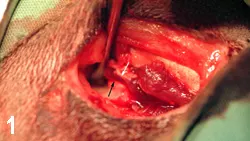

The ProcedureThe TMJ was approached through a lateral skin incision along the caudoventral margin of the zygomatic arch. A periosteal elevator was used to lift the condylar head (Figure 1; black arrow) into the temporal fossa (white arrow). The masseter muscle was reflected ventrally, and the damaged TMJ joint capsule was visualized by having an assistant open and close the jaw. The dorsocranially deviated condyle was reduced into the temporal fossa. A small hole was drilled through the lateral condyle and fossa by using a no. 1 round bur in a high-speed dental handpiece. A 4-0 nonresorbable nylon was threaded through the predrilled holes, and a simple interrupted knot was tied (Figure 2). Because there was no overlying musculature around the severely damaged joint capsule, imbrication was impossible. A postreduction extraoral radiograph indicated successful reduction (Figure 3).

A rostral incision was made along the mucogingival line, and the alveolar mucosa was reflected ventrally off of the symphysis. A small hole was predrilled on either side of the symphysis, and an intraosseous no. 24 gauge wire was placed and tightened to reduce the symphyseal fracture (Figure 4). The height of the incisors was used to determine whether reduction was adequate. The alveolar mucosa was reattached at the mucogingival line. The lower canines were acid-etched with a 37% phosphoric acid gel, rinsed, and dried. A self-mixing, autopolymerizing composite resin was then applied to the etched enamel of the lower canines for rigid fixation (Figure 5).

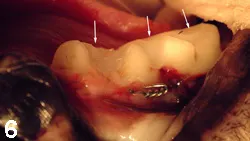
After alignment and stabilization of the anterior and the posterior portions of the left mandible, the mandibular fracture was then openly reduced. All granulation tissue was debrided from the site, and fracture fixation was accomplished with a full horizontal intraosseous cerclage wire. During tightening of the wire, a small stair-step height discrepancy was noticed between the 4th premolar and the 1st molar, but did not cause malocclusion or trauma to the soft tissue as monitored before and after surgery. The gingiva was then repositioned and sutured. The inside or lingual surface of the caudal cheek teeth (white arrows) was again prepared as above for a lingually placed autopolymerizing composite resin (Figure 6). Intraoral postoperative mandibular occlusal views were taken of the symphysis and the caudal ramus (Figures 7 and 8).
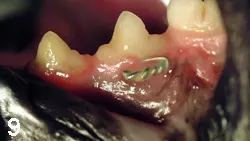
The ResultsAfter monitored recovery, the animal was sent home and the owner was instructed to feed the cat soft food and to flush the splints daily with diluted chlorhexidine solution. On physical presentation at the planned 8-week recheck for splint and wire removal, the gingiva was a normal pink and had grown around the cerclage wire (Figure 9). The jaws were aligned, and there was no evidence of dental malocclusion. The intraoral splints had fallen off by themselves. The radiographs indicated normal fracture healing (Figure 10). The caudal ramus wire was removed.
ORAL TRAUMA • Ira R. Luskin
Suggested Reading
Trauma to oral structures. Weigel JP. In Harvey CE (ed): Veterinary Dentistry, 1st ed-Philadelphia: WB Saunders, 1985, pp 141-155.Use of maxillary and mandibular splints for restoration of normal occlusion following jaw trauma in a cat. Legendre LFJ. J Vet Dent 15:179-181, 1998.