Oral Bone Infection
History. A 7-year-old, neutered male Scottish terrier was presented for professional teeth cleaning because of the owner's complaint of severe halitosis, which was described as being worse than "regular bad dog breath." Physical examination and preoperative laboratory tests, including a CBC and chemistry profile, were within normal limits. General anesthesia was induced and maintained with isoflurane (2% to 3%) and oxygen. Intravenous fluids were administered at 10.0 ml/kg/hr.
Oral Examination. The dog had severe halitosis with gross signs of stomatitis (Figure 1). Devitalized, necrotic bone (sequestrum) was associated with the mandibular left fourth premolar (308), first molar (309), and second molar (310), marked by periodontal bone destruction; the remaining bone appeared denuded and discolored (Figure 2a). Ulceration of adjacent oral mucosa was indicative of stomatitis. The lip commissure was tight bilaterally, making it difficult to visualize the mandibular first molar during caudal digital traction on the lips. Stomatitis of the right caudal oral cavity was noted; however, there were no signs of destructive periodontal disease or bone sequestrum. Intraoral dental radiographs of the left caudal mandible showed signs of radiolucent areas, bone destruction, and sequestrum formation (Figure 2b).

Figure 1. Oral photograph showing purulent fluid in the area of the mandibular left fourth premolar and first molar.

Figure 2. Oral photograph (a) showing bone sequestrum (arrows) in the area of the mandibular left fourth premolar, first molar, and second molar. Note the radiographic signs of bone lysis and radiolucent area (b;arrowheads) ventral to the sequestrum.
ASK YOURSELF ...On the basis of the clinical and radiographic findings, what is the most appropriate treatment plan?A. Extraction of the mandibular left fourth premolar, first molar, and second molar
B. Extraction of the mandibular left fourth premolar, first molar, and second molar, plus wound closure to revascularize the bone sequestrum
C. Extraction of the mandibular left fourth premolar, first molar, and second molar, and sequestrectomy
D. Extraction of the mandibular left fourth premolar, first molar, and second molar; sequestrectomy; and reconstructive surgery to alleviate the tight lip commissure
Correct Answer: CExtraction of the mandibular left fourth premolar, first molar, and second molar, and sequestrectomy
Treatment. Regional anesthesia was administered by injecting 0.5 ml of bupivacaine in the area of the alveolar nerve as it enters the caudal mandible at the mandibular foramen.
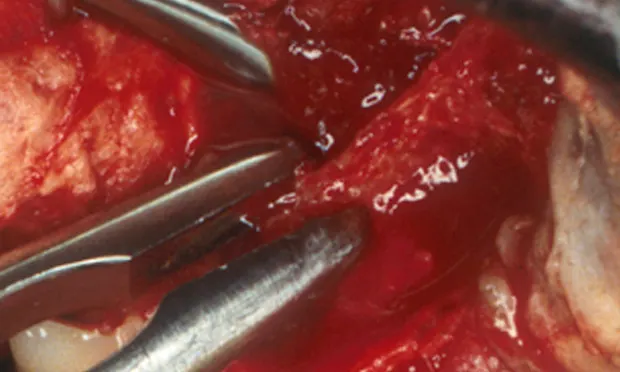
Commissurotomy was done to provide access to the teeth of the left caudal mandible. A mucoperiosteal flap was elevated by performing an interdental incision from the mandibular left fourth premolar to the second molar, followed by a vertical releasing incision at the distal line angle of the mandibular left third premolar (307). The mobile second molar was extracted. The mandibular left first molar and second molar received crown sectioning after initial sequestrectomy (Figure 3). The crown and root segments were elevated and extracted (Figure 4).
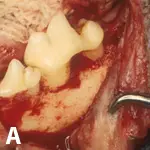
Figure 3. Intraoperative oral photograph (a) after initial sequestrectomy and extraction of the mobile mandibular left second molar. Debridement of necrotic bone (b;arrowheads) was followed by crown sectioning of the mandibular left fourth premolar and first molar to facilitate extraction.
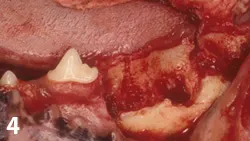
Figure 4. Intraoperative oral photograph taken after sequestrectomy and extraction.
Additional sequestrectomy and alveolectomy were done, followed by lavage with 0.12% chlorhexidine and wound closure with absorbable suture in a simple interrupted pattern (Figure 5). The commissurotomy was apposed in three layers with absorbable suture in a simple interrupted pattern and nonabsorbable suture for skin closure (Figure 6).


Figure 5. Intraoperative oral photographs showing additional bone debridement using bone rongeurs (a), followed by alveolectomy along the lingual aspect using a high-speed handpiece and round bur (b). The sequestrectomy and extraction sites (c) were lavaged with 0.12% chlorhexidine followed by wound closure using absorbable suture in a simple interrupted pattern (d)
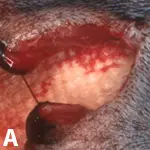
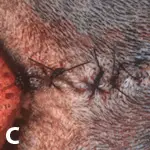
Figure 6. Photographs showing commissurotomy wound closure in three layers, beginning with the mucocutaneous junction (a) and followed by mucosal apposition (b) and skin closure (c).
Results. After surgery, the dog received a fentanyl patch for analgesia and therapy with an antiinflammatory (carprofen) and an antimicrobial (clindamycin). Bacterial culture and sensitivity testing were not done because of the expected polymicrobial outcome. Clindamycin was administered for 4 weeks on the basis of its effectiveness against pathologic organisms of the oral cavity and bone absorption. A negative clinical outcome would have warranted a percutaneous paramandibular aspirate using aseptic technique in an attempt to identify a causative agent. In this case, the 1-month postoperative examination indicated resolution of the stomatitis and routine healing of the oral wounds and the commissurotomy (Figure 7).

Figure 7. Photographs taken 2 months after surgery showing uncomplicated healing of the commissurotomy (a) and resolution of stomatitis (b).
TAKE-HOME MESSAGES
Halitosis that is considered worse than the usual "bad" dog breath may be a sign of bone infection and sequestrum.
Check the dog for associated stomatitis and a lip commissure that seems "tight" compared with that of other dogs.
Chronic stomatitis may lead to scar tissue formation and a seemingly tight commissure, or abnormal lip conformation may cause severe periodontal disease and secondary bone infection if it results in accumulation of food and debris in the caudolateral vestibule. Further objective data are needed to determine whether abnormal lip conformation occurs and is a predisposing factor.
Treatment must include sequestrectomy and extraction of associated teeth; antimicrobial therapy is ineffective without debridement of the necrotic bone; loss of periodontal bone support necessitates tooth extraction.
Sequestrectomy must be complete while the integrity of the cortical bone of the ventral mandible is maintained.
Reconstructive surgery to modify the lip commissure is unlikely to be effective and does not alter the treatment plan.
Oral bone infection and sequestrum formation may be secondary to fracture, periodontal disease, or radiation therapy; although rare, in this case bone infection and sequestrum formation were considered secondary to chronic periodontal disease.