Open & Laparoscopic Liver Biopsy
J. Brad Case, DVM, MS, DACVS, University of Florida
W. Alex Fox-Alvarez, DVM, MS, DACVS-SA, Community Care Veterinary Specialists, Gainesville, Florida
Liver biopsy is indicated when clinical signs, biochemical markers, and/or diagnostic imaging suggest hepatic disease. Biopsy allows definitive diagnosis of neoplastic, infectious, inflammatory, vascular, and mineral storage disease processes. With careful attention to patient evaluation and preparation, it can be performed safely in most animals. Complete blood count, serum chemistry panel, coagulation panel, urinalysis, and abdominal ultrasonography are often performed before biopsy.
In addition to general systemic health, coagulation ability should be evaluated. Although many animals with liver disease may have primary and/or secondary hemostatic abnormalities, liver biopsy can usually be performed safely, provided the clinician uses sound judgment and methodology.
Patients with significant coagulation abnormalities may benefit from plasma administration immediately before or the night before the surgical procedure. Dogs with von Willebrand factor deficiency should be pretreated with cryoprecipitate, plasma, or arginine vasopressin. Vitamin K can also be administered before the procedure. Medical textbooks may provide specific recommendations.
Liver Biopsy Techniques
Hepatic biopsy can be performed via laparotomy, laparoscopy, or percutaneously. Percutaneous needle biopsy should be used and interpreted with caution, however, as morphologic diagnosis via percutaneous biopsy may be inaccurate in a significant proportion of patients and controlled hemostasis is not possible.
Conversely, laparotomy and laparoscopy can expose most of the hepatic parenchyma, allowing for biopsy in most regions of the liver. While laparotomy is simple and requires no advanced instrumentation, it necessitates a large incision and is associated with greater patient morbidity as compared with laparoscopy. Laparoscopic liver biopsy is a safe and minimally invasive method of collecting diagnostic samples while reducing tissue trauma and patient morbidity.
Many liver biopsy techniques have been described. This article offers a quick reference on obtaining a liver biopsy sample using the Baker punch method via laparotomy and the clamshell technique via laparoscopy.
Related article: Surgeon's Corner: Visceral Biopsy Technique
Patient Positioning
For Baker punch biopsy, the patient should be in dorsal recumbency and the abdomen prepared using standard aseptic technique. If only the liver is to be biopsied, then a more limited cranial celiotomy approach may be taken. Neoplasia is a common differential for hepatic disease, so exploring the entire abdomen to evaluate for pathology in other organs (eg, lymph nodes) may be indicated.
Dorsal positioning is also preferred for laparoscopic biopsy because it allows visualization of all liver lobes and spares injury to abdominal musculature.
What You Will Need
Supplies for Both Methods
Sterile sample containers
10% formalin for histopathology
Microscope slides for impression cytology
Absorbable gelatin sponge
Baker Punch Biopsy
4- to 5-mm Baker biopsy punch
General surgery pack
Balfour retractor

(1) 5-mm laparoscopic clamshell biopsy forceps; (2) 5-mm laparoscope 0°; (3) 5-mm trocar; (4) camera; (5) insufflation tubing; (6) light cable; (7) 5-mm laparoscopic blunt probe

Videolaparoscopy tower, including (1) monitor; (2) video capture; (3) CO2 insufflator; (4) xenon light source
Step-by-Step: Baker Punch Biopsy via Laparotomy
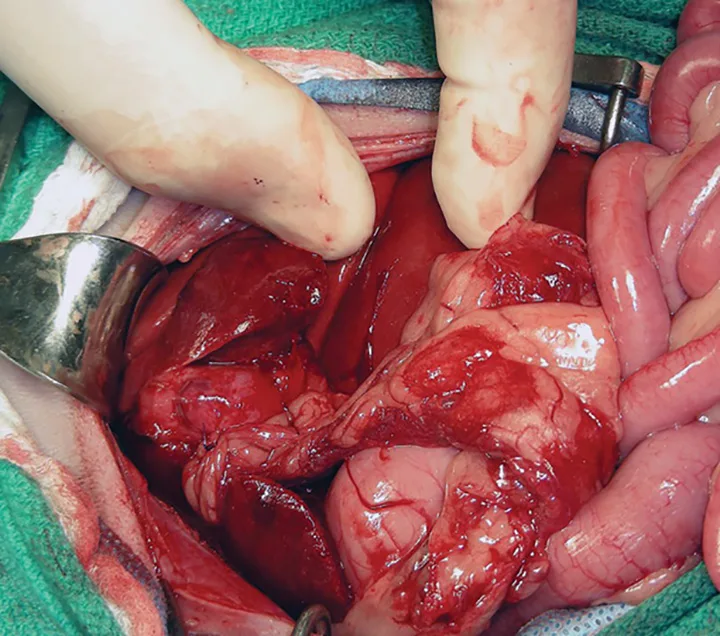
Step 1.
Perform a midline laparotomy from the caudal margin of the xiphoid process to the umbilicus. Excise the falciform fat to improve liver exposure. Place a selfretaining Balfour retractor. Evaluate abdominal viscera and peritoneal surfaces, and sample abnormal tissue for histopathology.
Author Insight
The nondominant hand can be used to retract the ventral surface of the liver caudally to improve exposure during biopsy.
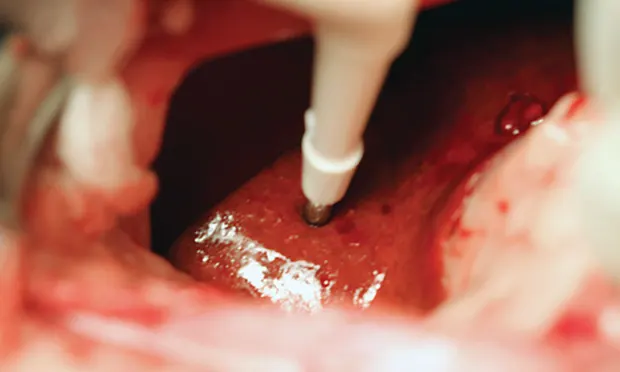
Step-by-Step: Clamshell Biopsy via Laparoscopy

Step 1A.
Make an incision no longer than the inner diameter of the cannula through the skin 1–2 cm caudal to the umbilicus (A). Continue the incision to the depth of the linea alba.