Open & Laparoscopic-Assisted Incisional Gastropexy

Gastric dilatation–volvulus (GDV) is a life-threatening medical and surgical emergency. The acute medical crisis is brought on by massive gastric distension, which compresses critical vasculature, causing gastric ischemia, impaired venous return, and poor cardiac output. This leads to hypovolemic shock, myocardial ischemia, cardiac arrhythmia, electrolyte imbalance, visceral necrosis, and other detrimental effects.
Related Article: Belt-Loop Gastropexy for Gastric Dilatation Volvulus
Large- and giant-breed dogs, underweight dogs, and dogs with a large thoracic depth:width ratio are at greater risk for developing GDV. This risk increases with age. One study found large and giant purebred dogs to have a lifelong risk for developing GDV of 24% and 21.6%, respectively.1
What Is a Gastropexy?
Gastropexy is a surgical procedure that creates a permanent adhesion between the pyloric antrum and the right abdominal wall, preventing gastric volvulus. When used to treat patients with GDV, recurrence rates drop to less than 5% compared with more than 50% if no gastropexy is performed.2 In a recent study, at-risk dogs treated with prophylactic incisional gastropexy had no episodes of GDV after a mean follow-up time of 2 years—results that are the same as or better than those for other reported techniques.3
Several gastropexy techniques have been described, including incisional, belt-loop, circumcostal, tube, incorporating, gastrocolopexy, endoscopically assisted, laparoscopic-assisted, and laparoscopic gastropexy.4 The minimally invasive procedures employ an incisional gastropexy in their technique. The authors prefer the incisional gastropexy technique because it is relatively safe, effective, and technically simple to perform.3 Prophylactic gastropexy can be performed alone or at the same time as sterilization in at-risk breeds. This article serves as a reference for performing incisional gastropexy using both open and laparoscopic-assisted5 techniques.
Related Article: Surgeon's Corner: Surgical Management of Gastric Dilatation-Volvulus (GDV)
Patient Positioning
For both open and laparoscopic-assisted incisional gastropexy, the patient should be positioned in dorsal recumbency and the abdomen prepared using standard aseptic technique.
What You Will Need
For Open Incisional Gastropexy
Standard surgical pack
2-0 polydioxanone suture (PDS) or other monofilament absorbable suture of choice
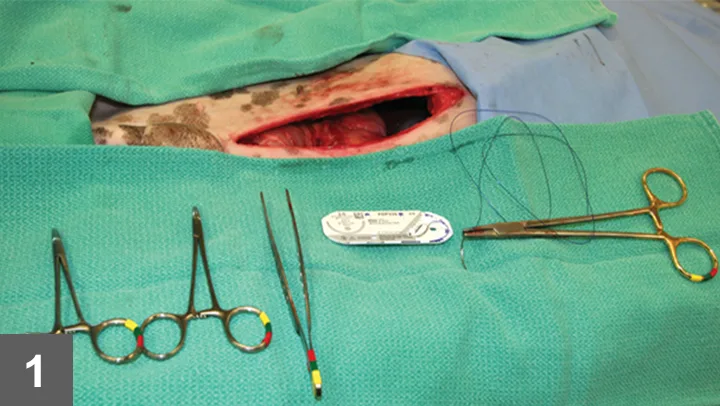
Step 1.
After standard abdominal draping, make a ventral midline abdominal incision extending from the xyphoid to 2–3 cm caudal to the umbilicus. Remove the falciform fat using electrosurgical dissection or ligation and en-bloc removal if necessary (not shown).
What You Will Need
For Laparoscopic-Assisted Incisional Gastropexy
Standard surgical pack
2-0 PDS or other monofilament absorbable suture of choice
#11 blade
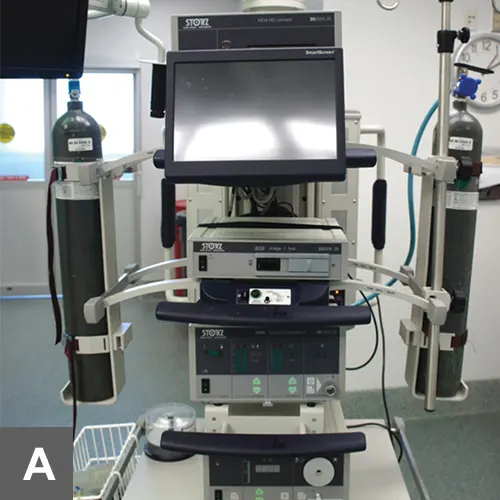
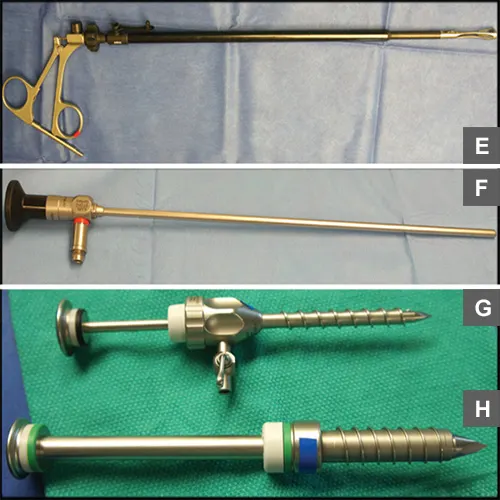
Video laparoscopy tower (A) with camera (B), insufflation tubing (C), light cable (D), and video capture device 10-mm laparoscopic Babcock forceps (E)
5-mm laparoscope 0° (F)
5-mm trocar (G) and 10-mm trocar (H)

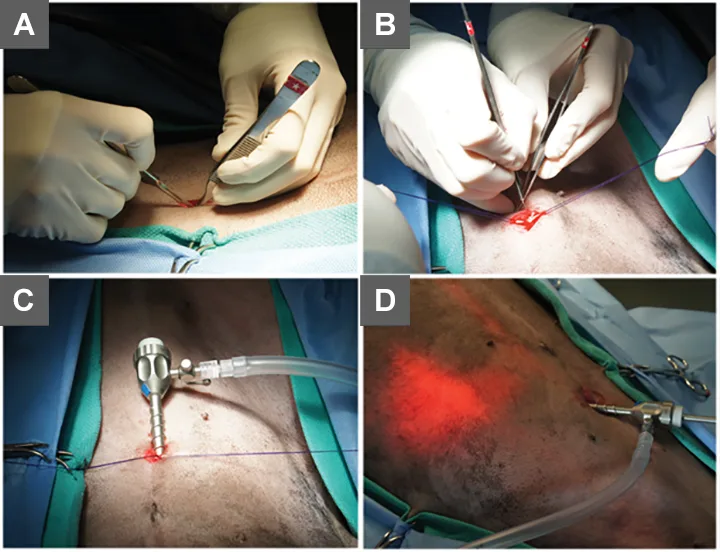
Step 1.
Using the modified Hasson technique, place a 5-mm cannula 1 to 2 cm caudal to the umbilicus on the midline as follows. Using a #11 blade, make an incision through the skin no longer than the inner diameter of the cannula (A). Continue the incision through the subcutaneous tissue into the linea alba. Place stay sutures in the linea to provide outward traction on the body wall while placing the port (B). Place a trocar–cannula assembly or threaded screw-in cannula through the incision and into the abdomen (C). Once the cannula is in place, attach CO2 insufflation tubing and pressurize the peritoneal cavity to a maximum 10 to 12 mm Hg. Insert the laparoscope into the cannula and observe the peritoneum briefly to ensure that no iatrogenic trauma or hemorrhage has occurred.
Author Insight
To avoid the cranial epigastric vasculature when making the next incision, use the laparoscope light to trans-illuminate the proposed site for the second port (D).