Nasal Swelling in a Border Collie
Josep Aisa, DVM, DECVS, University of Tennessee

Biscuit, a 3-year-old neutered male border collie, was presented with chronic and fluctuating localized swelling on the caudal aspect of the bridge of the nose. The swelling was first noticed by his owner when Biscuit was 4 months of age, but it did not appear to cause pain or discomfort.
The owner reported that the swelling ruptured 6 months prior to presentation, causing discharge of purulent exudate. This happened again on at least 2 additional occasions. Empiric systemic antibiotics prescribed at each flare appeared to aid in wound healing and resolved the discharge. There was no other relevant clinical history, and the owner did not report any apparent clinical signs of nasal disease (eg, nasal obstruction, rhinorrhea).
Physical Examination
Physical examination confirmed the presence of a fluctuating swelling 5 mm in diameter associated with a focal area of alopecia and scarring and located on the dorsal nasal midline 7 cm caudal to the nasal planum. On close inspection, a pinpoint draining tract (nasal pit) was also observed rostrally on the dorsal midline at the junction with the nasal planum (Figure 1). On gentle palpation of the caudal swelling, the rostral lesion discharged a small amount of purulent exudate. Biscuit exhibited mild discomfort on palpation of the swelling.
Biscuit was bright, alert, and responsive, and vital parameters were normal.
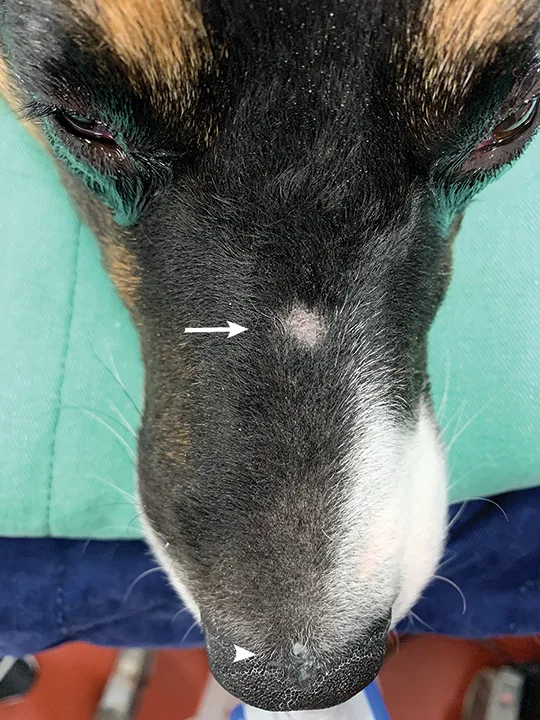
Gross appearance of the nasal lesions. Alopecia and scarring are present caudally (arrow), and a characteristic minute nasal pit can be seen at the junction with the nasal planum (arrowhead). Both lesions are located on the dorsal nasal midline. Purulent exudate can be seen around the nasal pit.
DIAGNOSIS:
NASAL DERMOID SINUS CYST
Diagnosis
A nasal dermoid sinus cyst was suspected based on patient age at initial presentation, clinical history, absence of reported trauma, chronicity, and findings on physical examination. The midline location of the lesion, as well as the presence and location of the nasal pit, are characteristic of nasal dermoid sinus cysts in dogs.1-6
Nasal dermoid sinus cysts in dogs are rare1-6 and are caused by ectodermal cell entrapment in the underlying mesoderm during early embryologic development. These cysts contain epidermal adnexa that produce hair and sebum and are therefore associated with an epithelium-lined sinus tract or cyst. Although the pathogenesis remains obscure, it is thought that the varying depth of nasal dermoids depends on the specific time when failure of embryologic development occurred. In dogs, these cysts often extend to the nasal septum1,2,4,5 and can reach the meningi.3,6 Patients can be presented with a discrete dorsal midline nasal swelling or a pit that may discharge hair or sebaceous material. Hair protrusion is pathognomonic of this condition.1,7 Fistulization may result from spontaneous rupture of the cyst or iatrogenically as a result of surgical intervention. Nasal dermoid sinus cysts may also become infected, with an increase in swelling and discharge of purulent material. Although clinical signs may be present at an early age, the condition may go unnoticed until later in life.
Differential diagnoses may include other forms of cysts (eg, epidermoid cyst without hair), chronic abscess, or pyogranulomatous reaction secondary to a retained foreign body (eg, fractured tooth fragment or vegetal material).
Routine hematology and serum chemistry tests were unremarkable. Findings on head CT (performed with the patient under sedation) included the presence of a mildly attenuating focal subcutaneous fluid and tissue swelling on the dorsal midline of the nose that continued caudoventrally through a defect of the nasal bone and caused moderate widening of the nasal septum (Figure 2). These findings were consistent with the tentative diagnosis of nasal dermoid sinus cyst. Contrast-enhanced CT is routinely performed in cases of suspected infection and was used to rule out cellulitis beyond the lesion in this patient. Plain radiography followed by positive contrast sinography is an alternative imaging modality to determine the extent of the dermoid cyst,1,2,5,6 although the contrast may not always reveal the full depth of the lesion. Use of MRI has been reported and is advised if intracranial extension of the lesion is suspected.3,4
Sampling of the lesion for bacterial culture and susceptibility testing was delayed until surgery so that a more representative deep tissue sample could be obtained.

FIGURE 2A
Precontrast, transverse plane CT image of the nasal passages at the level of the second premolars (A). There is an absence of complete closure of the nasal bone suture (arrows) and dilation of the most dorsal aspect of the nasal septal wall with soft tissue density (arrowhead). Precontrast, transverse plane CT image of the nasal passages at the level of the third premolars (B).
Treatment & Long-Term Management
The goal of surgery is to excise the entire tract, including all epidermal tissue, to eliminate risk for recurrence. All abnormal tissue was excised en bloc via dorsal nasal approach and limited dorsal rhinotomy. CT was used to determine the extent of the lesion and to aid in preoperative planning of the nasal and septal osteotomies that were performed with an oscillating saw (Figure 3). Soft tissue dissection was extended cranially to the level of the nasal pit, which was excised with the remaining tissue (Figure 4).
Alternative methods for excision of nasal dermoid cysts include a combination of blunt and sharp circumferential dissection and traction around the lesion,1,4,5 enlargement of the dorsal nasal suture defect via a more limited dorsal rhinotomy,2,6 and a transnasal endoscopic approach.<sup3 sup>
Biscuit recovered well from the procedure and was discharged the following day with carprofen (2.2 mg/kg PO every 12 hours) and gabapentin (15 mg/kg PO every 8 hours) after 12 hours of pure μ-agonist opioid medication (hydromorphone, 0.05-0.1 mg/kg IV every 4 hours). Tract tissue was submitted for histopathologic analysis and bacterial culture. Histopathology findings were consistent with nasal dermoid sinus lesion, and bacterial culture grew Staphylococcus pseudintermedius. Because the entire tract was removed en bloc, no antibiotic was prescribed postoperatively.
TREATMENT-AT-A-GLANCE
Antibiotics do not resolve nasal dermoid sinus cysts and can lead to a multidrug-resistant bacterial infection.
Complete surgical excision of the entire tract with clear margins is the treatment of choice. Cure should be expected after complete excision.
Incompletely excised nasal dermoid sinus cysts in human children are reported to reoccur in 50% to 100% of cases.8 Although similar information is not available in the veterinary literature, the recurrence rates may be similar in dogs, as revision surgery has been commonly reported.1,3,6
Circumferential dissection of the fistulous tract and sinus is recommended for superficial lesions.
Limited dorsal rhinotomy may be required for tracts that extend into the nasal planum. The normal turbinate anatomy should be preserved, if possible.
Prognosis & Outcome
Postoperative nasal bleeding was minor and subsided within 12 hours. No other complications were reported on follow-up one year after surgery.
Prognosis is typically excellent after complete excision of nasal dermoid sinus cysts and associated sinus tracts.1-6
TAKE-HOME MESSAGES
Nasal dermoid sinus cysts are rare congenital malformations in dogs that are caused by embryologic entrapment of ectoderm in deeper tissues and are often diagnosed in young dogs as swelling or discharge of purulent exudate on the dorsal midline of the nose.
A nasal pit at or near the junction between the haired and nonhaired skin of the nose on the dorsal midline is characteristic of this condition. A nasal pit or cyst with hair is pathognomonic.1-4
Nasal dermoid cysts have not been associated with other congenital abnormalities in dogs.
A presumptive diagnosis can be made based on the patient’s age at onset of clinical signs, specific midline nasal location of the draining tract and swelling, chronicity of the lesion, and absence of known trauma.
Diagnostic investigation can include positive contrast sinography, CT, or MRI to determine the true extent of the lesion and help with appropriate surgical planning. Lesion extension into the nasal septum is common, and CT can help direct surgical dissection to obtain a complete excision.