The Many Types of Shock
Garret E. Pachtinger, VMD, DACVECC, VETgirl; Veterinary Specialty and Emergency Center, Levittown, Pennsylvania

Shock, a syndrome in which clinical deterioration can occur quickly, has many causes, each one requiring careful analysis and rapid treatment. Broad definitions for shock include inadequate cellular energy production or the inability of the body to supply cells and tissues with oxygen and nutrients and remove waste products. Without rapid intervention, shock ultimately leads to cell death. Although hypovolemic shock is the most common clinical form of shock, other forms of shock include cardiogenic shock, distributive shock, obstructive shock, hypoxic shock, and metabolic shock. Determining type of shock can be complicated, as not only are there are many forms of shock, but their definitions overlap.
Related Article: Shock Fluid Therapy in Cats
Hypovolemic or Circulatory Shock
Hypovolemic or circulatory shock is the most common cause of shock seen in small animal practice. Hypovolemic shock results from a decreased intravascular volume, and causes commonly include hemorrhage, severe dehydration, and hypoproteinemia. Intraabdominal hemorrhage (Figure 1) may occur as a result of a ruptured splenic or hepatic mass, a coagulopathy, or trauma. Severe dehydration may be seen with prolonged fluid losses, as can be seen with vomiting and/or diarrhea.

Figure 1 Ultrasound image: peritoneal effusion and splenic mass
Patients with hypovolemic shock present with such signs as pale mucous membranes (Figure 2), prolonged capillary refill time (CRT), tachycardia, and poor pulse quality. Treatment includes rapid administration of IV fluids and may include isotonic crystalloids, hypertonic crystalloids (eg, 7.5% NaCl), synthetic colloids, or blood products.

Figure 2 Triage examination with a concern for pale-white mucous membranes
Cardiogenic Shock
As compared with the decreased intravascular fluid volume in hypovolemic shock, cardiogenic shock is a failure of the heart pump associated with a normal to increased intravascular volume, leading to decreased cardiac output. Causes include congestive heart failure, myocardial abnormalities (eg, dilated cardiomyopathy, hypertrophic cardiomyopathy), or cardiac arrhythmias. Treatment (which typically does not include IV fluid therapy) depends on the underlying disease process: β-agonist therapy for decreased myocardial contractility (eg, dobutamine), diuretic therapy for excessive preload (eg, furosemide), or therapy to reduce afterload in cases of severe valvular disease (eg, nitroprusside). Patients with cardiogenic shock often have unique examination findings (eg, tachypnea, dyspnea, auscultation of abnormal lung sounds [pulmonary crackles]) to help differentiate this shock type from others.
Distributive Shock
Distributive shock is often seen as a relative hypovolemia, resulting from a maldistribution of blood flow despite adequate total body fluid volume. Causes of distributive shock include Systemic Inflammatory Response Syndrome (SIRS), sepsis, and anaphylaxis. Treatment is complex and warrants identification of the underlying disease process to provide goal-directed therapy, which may include IV fluid therapy, vasopressors, and inotropic therapy. Hemodynamic changes in distributive shock can be subdivided into early or late phases. Examination findings in early distributive or septic shock are characterized by peripheral vasodilation that causes bright (brick) red mucous membranes, a rapid (<1 second) CRT, tachycardia, and hyperdynamic femoral pulses. In late distributive shock, peripheral vascular paralysis results in hypoperfusion, characterized by pale mucous membranes, tachycardia, and poor femoral pulse quality.
Related Article: Synthetic Colloid Fluids & Volume Expansion
Obstructive Shock
Obstructive shock is caused by any obstruction or maldistribution of blood flow that results in a decreased preload and subsequent decreased cardiac output. Causes of obstructive shock include gastric dilatation–volvulus (GDV), caval syndrome from heartworm disease, and pericardial effusion (Figure 3). Therapy involves identification and correction of the underlying cause of the obstruction—for example, stomach decompression in GDV or pericardiocentesis for pericardial effusion. Similar to hypovolemic shock treatment, IV fluid therapy can be beneficial for cases of obstructive shock.

Figure 3 Ventrodorsal thoracic radiograph with severe, globoid cardiomegaly
Hypoxic Shock
Hypoxic shock is seen with normal tissue perfusion but decreased oxygen content of arterial blood. The equation for oxygen content is:
CaO2 = Hb (gm/dl) x 1.34 ml O2/gm Hb x SaO2 + PaO2 x (.003 ml O2/mm Hg/dl)
The value in understanding this equation and its relationship with hypoxic shock is that tissues need a requisite amount of oxygen for normal metabolism. Neither the PaO2 nor the SaO2 provide information on the number of oxygen molecules in the blood. Of the three values used for assessing blood oxygen levels (ie, CaO2, PaO2, and SaO2), CaO2 is the only value that has a measure of units, notably O2/dl. This is because CaO2 is the only value that incorporates the hemoglobin content.
The most common causes of hypoxic shock include pulmonary disease resulting in a low partial pressure of arterial oxygen and anemia resulting in low levels of hemoglobin, impairing oxygen delivery to the tissues. Treatment often begins with oxygen therapy; however, if severe anemia is present, oxygen therapy alone will not be sufficient to increase the oxygen content of the blood. Patients with hypoxic shock as a result of severe anemia will require a blood transfusion to improve the overall oxygen carrying capacity of the blood.
Metabolic Shock
Metabolic shock is seen when the tissues receive the appropriate perfusion, nutrients, and oxygen delivery, but the cells are unable to utilize these fuel sources. Causes for metabolic shock include cyanide toxicity, cytopathic hypoxia of sepsis (Figure 4), and hypoglycemia. Diagnosis and treatment of the specific underlying cause will direct therapy. For example, hypoglycemia can be rapidly diagnosed with a glucometer and quickly treated with dextrose supplementation. Other forms of metabolic shock, including cyanide toxicity, are more difficult to diagnose and treat.
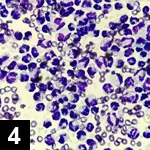
Figure 4 Cytology: severe suppurative, neutrophilic effusion: 100X oil
Conclusion
The goals in diagnosis and treatment of shock are to decrease patient morbidity and mortality by optimizing perfusion and oxygen delivery, improving the ability of cells to utilize these nutrients.