Limitations of Oral Examination in the Conscious Patient
Ana Nemec, DVM, PhD, DAVDC, DEVDC, University of Ljubljana, Ljubljana, Slovenia
Rod Jouppi, DVM, Laurentian University, Ontario, Canada
Brook A. Niemiec, DVM, DAVDC, DEVDC, FAVD, Veterinary Dental Specialties & Oral Surgery, San Diego, California
Paulo V. Steagall, DVM, MS, PhD, DACVAA, Université de Montréal, Quebec, Canada

Assessment of the oral cavity in the conscious patient can lead the clinician to underestimate the extent and severity of oral and dental disease. The following case demonstrates the need for detailed periodontal probing and dental charting, supported by dental radiographs, to fully evaluate oral and dental health, possible association with nasal disease, and appropriate treatment plans.
THE CASE
A 10-year-old, 15-lb (7-kg) male crossbreed dog was referred for diagnostic investigation due to sneezing and chronic unilateral nasal discharge that responded temporarily to administration of antibiotics and NSAIDs. The dog had recently been diagnosed via echocardiography with Stage B1 chronic valvular heart disease (ie, myxomatous mitral valve disease)1 but had no other health concerns. Dental cleaning had been performed twice yearly for the past 4 years without general anesthesia; no other at-home oral care was performed. The details of the nonanesthetic dental cleaning procedure were unknown to the owner, but the owner was informed about 2 mobile incisor teeth during the last procedure. The remaining teeth were determined to be in good condition for a 10-year-old dog.
Diagnostics
A grade II/VI heart murmur and purulent left nasal discharge were noted on physical examination; the remainder of the examination was unremarkable. Oral examination of the conscious patient revealed missing left and right maxillary first and second premolar teeth and generalized moderate plaque and calculus accumulation. Mobility and gingival recession at the right maxillary first and second incisor teeth were noted when the lip was lifted and were suggestive of advanced periodontitis. CBC revealed mild leukocytosis (17 900/μL; reference range, 4000-15 500/μL). Serum chemistry profile and urinalysis results were within normal limits.
Premedication was performed with methadone (0.5 mg/kg IM) and midazolam (0.25 mg/kg IM). General anesthesia was induced with alfaxalone (2 mg/kg IV), followed by endotracheal intubation, and maintained with isoflurane in oxygen. Because antibiotic treatment was started again 2 days before the procedure, ampicillin (20 mg/kg IV) was administered after induction in addition to carprofen (4 mg/kg SC). Monitoring included ECG, pulse oximetry, noninvasive blood pressure monitoring, and capnography. A balanced crystalloid solution (1.5 mL/kg/hr IV) was administered.

With the patient under general anesthesia and in dorsal recumbency, dental charting and periodontal probing were performed on a tooth-by-tooth basis and revealed advanced periodontitis (PD4) at the right maxillary first and second incisor teeth and both maxillary canine teeth, with an oronasal fistula at the left maxillary canine tooth. The periodontal probe can be seen “disappearing” into the deep periodontal pocket/into the nose, which is characteristic of an oronasal fistula.
The oral cavity was rinsed with 0.12% chlorhexidine solution, and a complete oral examination using a UNC-15 periodontal probe and dental explorer was performed and supported by full-mouth dental radiographs. Detailed oral examination with the patient under general anesthesia confirmed bilaterally absent maxillary first and second premolar teeth (previously noted) with apparently intact soft tissue in the areas of missing teeth. Generalized moderate plaque and calculus accumulation were also confirmed and were associated with generalized moderate gingivitis. Mobility of 2 (ie, mobility over a distance of more than 0.5 mm and up to 1 mm)2 at the right maxillary first incisor tooth and mobility of 3 (ie, mobility over a distance exceeding 1 mm)2 at the right maxillary second incisor tooth with gingival recession of 4 mm and probing depth of 6 mm were diagnosed, confirming suspicion of advanced periodontitis. Physiologic mobility of a tooth is considered to be up to 0.2 mm, and normal/sulcal probing depth in a dog this size would be expected to be 1 to 2 mm.2 In addition, probing depth was >15 mm at the mesiopalatal aspect of the left maxillary canine tooth (Figure 1), which also had mobility of 1 (ie, mobility over a distance >0.2 mm and ≤0.5 mm)2; this had not been previously noted on the conscious examination. Bleeding from the left nostril occurred, which was suggestive of an oronasal fistula, likely the cause of the chronic unilateral nasal discharge. Probing depth at the mesiopalatal aspect of the right maxillary canine tooth was noted to be 10 mm, indicating advanced periodontitis at this tooth as well. The rest of the dental charting was within normal limits. Dental radiographs confirmed the clinical findings and revealed a retained root tip in the area of missing teeth (Figure 2).

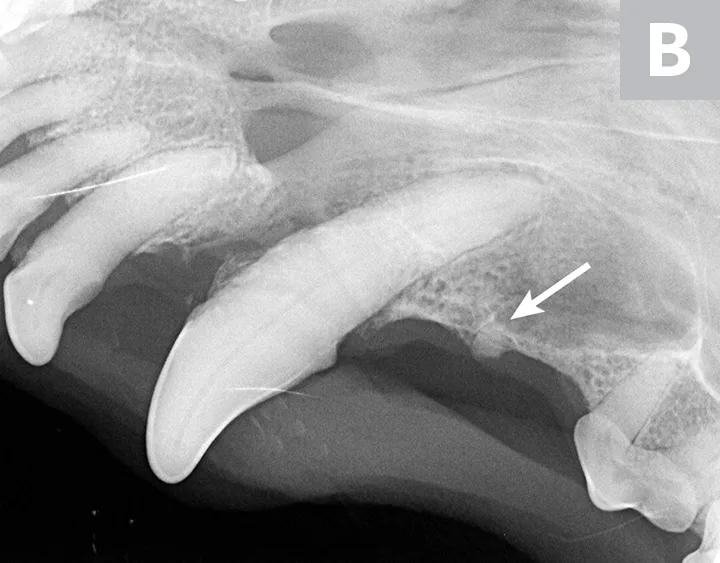
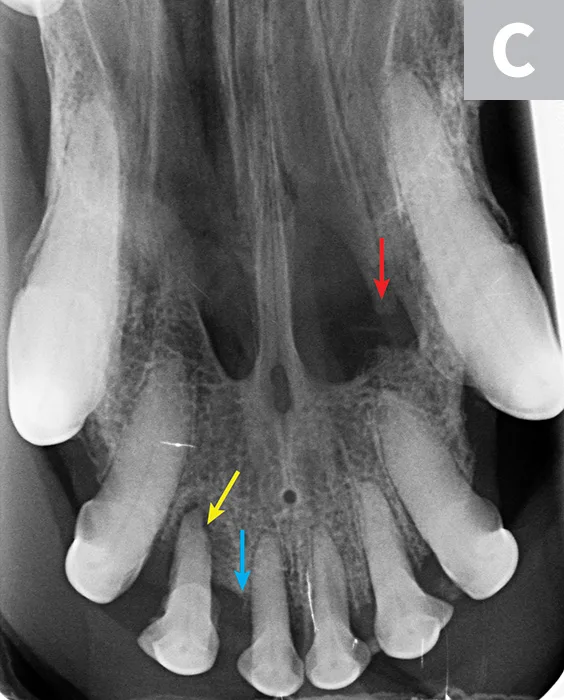
Dental radiographs of the right (A) and left (B) maxillary canine teeth (lateral views) and the rostral maxillae (C; occlusal view) confirmed mild horizontal and severe vertical bone loss at the mesial aspect of both maxillary canine teeth. Moderate to severe horizontal bone loss at the right maxillary first incisor tooth (blue arrow) and total loss of attachment with inflammatory root resorption at the right maxillary second incisor tooth (yellow arrow) were present. The remaining maxillary incisor teeth were affected by mild horizontal bone loss. Although the occlusal view of the rostral maxillae is slightly asymmetric, osteolysis was evident in the area of the left palatine fissure (red arrow). Mild horizontal bone loss was diagnosed at several other teeth. In addition, retained root tip of the left maxillary (presumably) first premolar tooth (white arrow) was identified.
Treatment & Follow-Up
Dental extractions of the severely periodontally affected teeth and the retained root tip—to remove the source of nasal disease, infection, and pain—were performed following infraorbital nerve blocks3 with 0.25% levobupivacaine (0.5 mL) and dental cleaning. The right maxillary first and second incisor teeth were removed via closed extraction.4 Surgical extraction (triangular flaps) was performed on the maxillary canine teeth5 with the incision extended on the left to the level of the retained root tip, which was also removed. Surgical sites and the nasal cavity on the left were copiously flushed with sterile saline and debrided of unhealthy bone and soft tissue before closure; a single-layer technique was used to repair the oronasal fistula.6
The dog recovered uneventfully after receiving a second dose of methadone (0.3 mg/kg IV) and was discharged the same evening with carprofen (4 mg/kg PO q24h for 7 days) and topical chlorhexidine mouthwash. Amoxicillin–clavulanic acid (20 mg/kg PO q12h for 10 days) was used to complete the previously started antibiotic course but was also deemed beneficial to treat severe infection of the tissues noted on removal of the left maxillary canine tooth, as well as the previously noted mild leukocytosis. At a 2-week recheck examination, the surgery sites appeared healed and the owner reported resolution of sneezing and nasal discharge.
Discussion
Oral examination should be a part of every physical examination, especially in dogs with chronic nasal disease.7-9 Oral examination in a conscious patient provides limited information; thus, a complete oral examination, including dental radiography with the patient under general anesthesia, is required to fully evaluate oral/dental diseases.10-17 If the cause of nasal disease cannot be attributed to dental/periodontal disease, CT and rhinoscopy should be performed.18
Patients with systemic disease should undergo a thorough physical examination, and additional diagnostic procedures may be required prior to general anesthesia. Systemic diseases are not contraindications for general anesthesia, and specialists in anesthesiology and pain management can be consulted to create an optimal anesthetic protocol. Avoiding anesthesia in dental patients may lead to incorrect or missed diagnoses and delayed treatment, resulting in prolongation of pain and progression of oral/dental disease(s).13-17
Appropriate surgical management of severe periodontitis and an oronasal fistula4-6 will most likely result in prompt resolution of clinical signs, as in this case. Although supportive analgesic and local antiseptic treatment are mandatory, use of antibiotics in veterinary and human dental patients is highly debated and should be minimized.19,20 In this case, severe local infection and systemic response (ie, leukocytosis) led the clinician to treat the patient with a broad-spectrum antibiotic.
Conclusion
This case demonstrates the limitations of an oral examination in a conscious patient, which can lead to underdiagnosing of oral/dental diseases and therefore inappropriate treatment. Anesthesia-free dental procedures often contribute to poor animal welfare, as such procedures may actually contribute to tissue damage and discomfort and pain to the animal without a meaningful result. Pet owners may believe that anesthesia-free dental treatment is sufficient and thus delay appropriate treatment, which can lead to progressive health issues that could negatively affect their pet’s welfare. For more information about the risks of anesthesia-free dentistry, see Suggested Reading.