Lethargy, Inappetence, & Increased Respiratory Effort In A Cat

A 5-year-old, neutered male domestic short haired cat was presented for evaluation of a 48-hour history of lethargy, inappetence, and increased respiratory effort.
HISTORYReduced interaction and hiding behaviors were noted by the owner about 2 days before presentation. The cat had not eaten in 24 hours and had an increased abdominal component to its respirations. The cat had been healthy, was on no medications, and had received scheduled vaccinations 15 months earlier; at that time the examination was unremarkable.
EXAMINATIONThe cat was alert, responsive, and hydrated, with pink mucous membranes and normal capillary refill time. Mild dental disease was noted.
The heart rate was 170 beats/min and regular. An extra diastolic heart sound was detected, but no murmur was evident. Femoral pulses were strong and synchronous. The jugular venous pulse was normal. The respiratory rate was 32 breaths/min with a mild increase in effort. Bronchovesicular sounds were increased over all lung fields.
DIAGNOSTICSDual-view radiographs (see Figure 1 below) and an ECG (see Figure 2 below) were obtained at presentation.

Figure 1. Dorsoventral (A) and right lateral (B) radiographs.
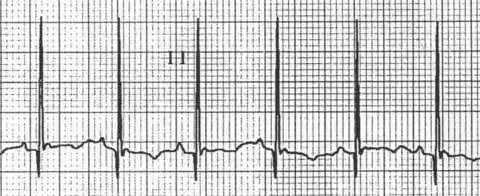
Figure 2. Lead II ECG (50 mm/sec; standard sensitivity) with the cat in right lateral recumbency. The heart rate is 230 beats/min, which is faster than the rate during examination, likely due to stress from being restrained for the ECG.
Ask Yourself...
What examination, ECG, and radiographic findings suggest heart disease?
What treatment if any should be instituted based on the initial diagnostic findings?
What role might echocardiography play in reaching a diagnosis?
DIAGNOSIS: Feline cardiomyopathy consistent with restrictive cardiomyopathyThe ECG and radiographic findings were consistent with heart enlargement and congestive heart failure.
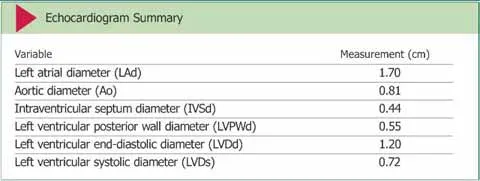
DEFINITIVE DIAGNOSISAn echocardiogram (see Figure 3 below) obtained 3 days after presentation demonstrated moderate to severe atrial enlargement, normal to mild left ventricular wall thickening, a normal left ventricular chamber, and a fibrous/fibromuscular band of tissue traversing the left ventricular lumen (see Echocardiogram Summary).
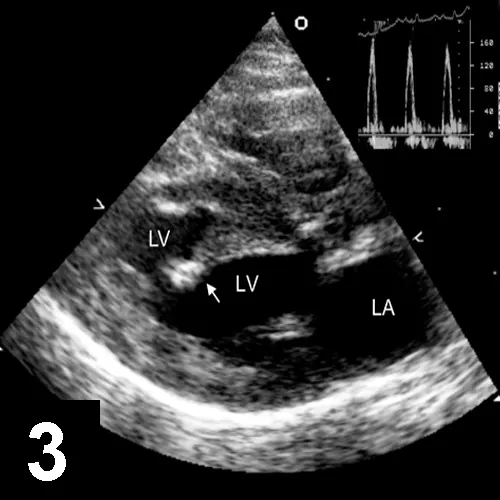
Figure 3. Right parasternal long-axis echocardiogram showing the left atrium (LA) revealed a fibrous band of tissue (arrow) spanning the LV cavity. The inset shows a spectral pulsed-Doppler tracing of transmitral inflow.
Doppler study of the diastolic mitral inflow revealed an elevated E:A ratio (between early and late ventricular mitral filling velocity), rapid deceleration time of the E-wave, and elevated mitral inflow velocity in the absence of significant mitral regurgitation. No blood flow gradient across the fibrous LV band was detected. These findings are most consistent with restrictive-type cardiomyopathy.
TREATMENTTreatment was initiated with the loop diuretic furosemide at 6.25 mg PO Q 12 H and the angiotensin-converting enzyme inhibitor (ACE-I) benazepril at 1.25 mg PO Q 24 H. Because both drugs have the potential to adversely affect renal function, a baseline renal panel was conducted before treatment was initiated and again 3 days later. Adverse reactions to either drug typically occur within 3 to 5 days of therapy initiation. Blood urea nitrogen (BUN) and creatinine levels before and after therapy were unremarkable (BUN—pretreatment, 27 mg/dL; posttreatment, 24 mg/dL; normal, 15–32 mg/dL; creatinine—pretreatment, 1.6 mg/dL; posttreatment, 1.4 mg/dL; normal, 1.0–2.0 mg/dL).
OUTCOMEThe cat’s respiratory rate and effort were normal 3 days after treatment was initiated, and according to the owner the cat was eating and acting normally. Re-evaluation of the patient, including physical examination, ECG, and echocardiogram, is indicated in 3 to 6 months. Thoracic radiographs are unlikely to be beneficial if the patient has no clinical signs consistent with decompensated congestive heart failure.
ACE-I = angiotensin-converting enzyme inhibitor; BUN = blood urea nitrogen; ECG = electrocardiogram
Did You Answer?
The extra heart sound on examination may have represented a diastolic gallop, as it was diastolic and of low frequency, which can indicate cardiac diastolic dysfunction. The ECG revealed sinus rhythm (heart rate, 230 beats/min) and increased R-wave amplitude (2.1 mV; normal <0.9 mV), which suggest left ventricular hypertrophy. The radiographs revealed generalized cardiomegaly, left atrial enlargement, distended and prominent pulmonary vasculature, and cardiomegaly with a patchy interstitial pattern. This combination of findings is most consistent with cardiogenic pulmonary edema.
The initial findings on presentation were sufficient to make a presumptive diagnosis of congestive heart failure. Regardless of the exact nature of the underlying disease, diuretics and ACE-I therapy should be prescribed to alleviate the signs of congestion.
Note that appropriate therapy was correctly started before echocardiography and that renal function was monitored. Antiplatelet therapy with aspirin at 81 mg PO Q 72 H or clopidogrel at 18.75 mg PO Q 24 H can also be considered in cats with enlarged atria in an attempt to lower the risk for thrombo-embolism.
In an emergency situation requiring patient hospitalization to receive supplemental oxygen and parenteral diuretics, some clinicians might administer topical nitroglycerin therapy at 1/8 inch to the pinna Q 8 H for 2 to 3 days. In addition, some clinicians elect to delay starting ACE-I therapy until the patient has been eating and drinking at home for several days after discharge.
The echocardiogram revealed a band of fibrous (or fibromuscular) tissue that spanned the left ventricular lumen, normal to mildly thickened left ventricular walls, and moderate to severe left atrial enlargement. Blood flow from the left atrium to the left ventricle was increased in velocity, which is consistent with altered left ventricular diastolic function and elevated left atrial pressure (ie, restrictive filling pattern). Although the echocardiogram provided a definitive diagnosis, depending on the history, clinical signs, as well as examination, ECG, and radiographic findings, echocardiography is not always necessary before initiation of therapy. Thus, the lack of immediate access to echocardiography does not automatically preclude the detection and initial treatment of congestive heart failure in cats.
For more on feline heart disease, see "Cardiac Disorder in a Cat," November 2008, at cliniciansbrief.com/journal