Kidney Disease in a Cat
Socks, an 11-year-old, 5.8-kg, castrated domestic shorthaired cat was presented for evaluation of suspected chronic kidney disease (CKD).
Clinical PresentationSocks appeared bright, alert, and responsive. He had a body condition score (BCS) of 2.5 out of 5, rectal temperature of 101.6°F, heart rate of 200 beats/min with strong regular pulses, and respiratory rate of 48 breaths/min. The hydration status was adequate. No abnormalities were detected on thoracic auscultation, but palpation revealed small, firm, irregular kidneys.
No enlargement of the thyroid glands was noted, and there were no abnormalities on funduscopic examination. The systolic blood pressure by indirect Doppler measurement was 135 mm Hg (normal, <160).
Laboratory FindingsLaboratory studies of blood, serum, and urine were conducted; the urine protein:creatinine ratio and blood urea nitrogen (BUN) and creatinine concentrations remained unchanged (Table 1, below) from laboratory studies obtained 2 weeks earlier.
Urinalysis was performed on a urine sample obtained by cystocentesis; culture was negative.
Table 1. Key Laboratory Findings
BUN = blood urea nitrogen, hpf = high-power field, RBC = red blood cells, UP:C = urine protein:creatinine
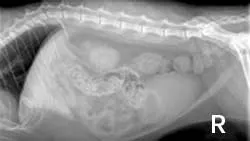
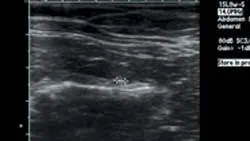
ImagingAbdominal radiographs showed small irregular kidneys (Figure 1, right: Radiograph of the right lateral abdomen. The kidneys are small and irregularly shaped. Mineral densities are visible in the left kidney. View larger image), and irregular margins were evident in ultrasound imaging (Figure 2, below: Ultrasound of the left kidney demonstrating irregular margins. View larger image).
Ask Yourself: According to the International Renal Interest Society (IRIS) CKD staging system, which stage of the disease does this patient have and what treatments are appropriate at this time?

A. IRIS CKD Stage 1 (nonazotemic, proteinuric, nonhypertensive); longitudinal monitoringB. IRIS CKD Stage 1 (nonazotemic, proteinuric, nonhypertensive); admit to the hospital and initiate diuresisC. IRIS CKD Stage 2 (mild renal azotemia, proteinuric, nonhypertensive); begin feeding low-protein diet +/- enteric phosphate binders, and because of proteinuria, consider administering angiotensin-converting enzyme (ACE) inhibitorD. IRIS CKD Stage 2 (mild renal azotemia, proteinuric, nonhypertensive); begin enteric dialysis
Answer**:** C. IRIS CKD Stage 2 (mild renal azotemia, proteinuric, nonhypertensive); begin feeding low-protein diet +/- enteric phosphate binders, and because of proteinuria, consider administering ACE inhibitor
Treatment for this cat included gradual introduction of a prescription renal diet and initiation of therapy with benazepril (2.5 mg Q 24 H). Follow-up examinations were scheduled every 30 days.
An appropriate serum phosphorus concentration for a cat with IRIS CKD Stage 2 is 2.5 to 4.5 mg/dL. If dietary therapy alone does not achieve this goal, enteric phosphate binders can be added to the treatment regimen.
Staging of Chronic Kidney DiseaseA standardized method of staging CKD based primarily on the serum creatinine concentration has been established to guide further diagnostic evaluation and treatment in cats (Table 2).
Table 2. Feline IRIS CKD stages
Before assigning a stage, 2 or more serum creatinine values should be obtained over several days or weeks to ensure that the disease process is stable.
To rule out pre- and postrenal causes of azotemia, the serum creatinine concentration must be interpreted in correlation with urine specific gravity and examination findings. The stages are further classified by the presence or absence of proteinuria and systemic hypertension (Tables 3 and 4).
Table 3. IRIS CKD Substaging (UP:C)
Table 4. IRIS CKD Substaging (systemic hypertension)
Staging at a Glance
CKD staging is based on evaluating serum creatinine concentration and confirming the degree of proteinuria and hypertension.
IRIS CKD Stages 1 & 2
Cats are often asymptomatic or have only mild clinical signs of kidney dysfunction.
Appropriate diagnostic evaluation should focus on the primary renal disease and longitudinal monitoring for disease progression.
Renoprotective treatments (eg, dietary therapy, enteric phosphate binders, ACE inhibitors for proteinuria and/or hypertension) are
usually initiated in IRIS CKD Stage 2.
IRIS CKD Stage 3
Cats typically show signs associated with loss of kidney function but usually without signs of uremia.
Renoprotective therapy for the prevention of disease progression is the primary treatment objective.
Treatment for alleviation of signs associated with renal dysfunction may be necessary.
IRIS CKD Stage 4
Cats have moderate to severe renal azotemia and signs of uremia may be present.
Treatment objectives include alleviation of clinical signs (eg, correction of dehydration, anemia, hypokalemia).
Feeding tubes and enteric dialysis may be beneficial.
Follow-UpAt the 3-month follow-up examination, Socks’ serum creatinine concentration was stable. The UP:C ratio was 0.3, BUN concentration 34 mg/dL, and serum phosphorus concentration 4.2 mg/dL.
Acute-Onset Anorexia & LethargyApproximately 4.5 months after initial evaluation, Socks presented with acute onset of anorexia and lethargy. Although he was quiet, his vital signs were within normal limits. He weighed 5.74 kg, his BCS was 2.5 out of 5, and the systolic blood pressure was 165 mm Hg.
Socks’ packed cell volume was 34%, UP:C ratio was unchanged (0.3), total protein concentration was stable (7.8 mg/dL), and BUN (62 mg/dL) and creatinine (6.4 mg/dL) concentrations had increased. Repeat culture of urine was negative.
Static left renal disease and mild hydronephrosis of the right kidney with proximal hydroureter were evident on renal ultrasonography (Figure 3, right: Ultrasound of the right kidney showing pelvic dilation. View larger image). Renal calculi were present bilaterally.

Socks was treated with 1.5 times maintenance IV fluids overnight. The following day, a renal profile revealed further increases in BUN (72 mg/dL) and serum creatinine (6.5 mg/dL) concentrations.
Ask Yourself: What is the most likely cause of Socks’ acute uremic crisis?A. Prerenal dehydrationB. Ascending infectionC. Disease progression associated with hypertensionD. Obstructive uropathy
Answer: D. Obstructive uropathy
Lack of response to fluid therapy and a negative urine culture make prerenal dehydration and an ascending infection unlikely. Socks’ increased blood pressure measurement was most likely a stress reaction to declining renal function.

Repeat ultrasonography and right-sided pyelocentesis with contrast confirmed right-sided hydronephrosis and hydroureter with no contrast progressing into the urinary bladder (Figure 4, above: Pyelogram identifying hydronephrosis of the right kidney and proximal hydroureter. Contrast material does not progress into the urinary bladder. View larger image). A ureterolith associated with the hydroureter was also visualized (Figure 5, below: Ultrasound identifying dilation of the right ureter associated with a ureterolith. View larger image).
These findings suggest the most likely cause of the uremic crisis was obstructive uropathy. Culture of the renal pelvic fluid yielded no bacterial growth.
Right-sided ureterotomy and cystotomy were performed and several stones were removed from the ureter. Socks recovered uneventfully, began eating, and was discharged from the hospital 4 days after surgery. On the day of discharge, his azotemia had improved (BUN concentration was 49 mg/dL and serum creatinine concentration was 3.2 mg/dL).
Take-Home Messages
IRIS CKD staging provides guidelines for further diagnostic evaluation and treatment.
In patients with early IRIS CKD Stage 2, diagnostic and treatment efforts should be directed toward monitoring renal function for stability/progression of disease and, if possible, identifying and treating the underlying primary renal disease.
Later in IRIS CKD Stage 2, when most CKD becomes progressive, renoprotective treatments become the major treatment focus.
The most common causes of an acute uremic crisis in a patient with previously stable CKD are prerenal dehydration, ascending infection, disease progression, and obstructive uropathy.
BUN = blood urea nitrogen, CKD = chronic kidney disease, IRIS = International Renal Interest Society
For related articles, see the following:Making Clinical Sense: CKD and SecondaryHypertensionManaging Canine Kidney Failure Through EBMLameness & Kidney Disease with B Burgdorferi