Identifying the Linea Alba & Avoiding Paramedian Incisions During Midline Celiotomy
Daniel D. Smeak, DVM, DACVS, Colorado State University
When performing midline celiotomy, properly identifying the linea alba and avoiding paramedian abdominal wall incisions are key to avoiding incising the rectus abdominal muscle (Figure 1). An acceptable midline incision should be made directly through the linea alba or medial to the rectus abdominal muscles and maintained throughout the approach to avoid muscle damage. A para-median incision is made off midline and involves incising the rectus abdominal muscle and exposing it on both sides of the incision (see Benefits of Midline Linea Alba Incision Versus Paramedian Incision).
The linea alba is a dense collagenous band found on the ventral midline of the abdominal wall extending from the base of the xiphoid process to the prepubic tendon (ie, cranial pubic ligament).1 Fascias of the transverse abdominal muscle and external and internal abdominal oblique muscles fuse on the midline to form this thick collagenous strip. Medial borders of the left and right rectus abdominal muscles are positioned closely against the lateral borders of the linea alba. The linea alba contains a palpable umbilical scar at the level of a transverse plane through the last rib. At its most cranial aspect, the linea alba is approximately 1 cm wide and less than several millimeters thick, gradually narrowing and thickening caudal to the umbilicus.2

Paramedian incision, linea alba incision, and an acceptable midline approach. Figure adapted from Anatomy of the Human Body, illustrated by Henry Vandyke Carter, used under fair use
Cats have a relatively wider, more transparent linea alba that is easier to visually identify as compared with dogs.
A plan should be made for creating the initial stab incision in the cranial aspect of the proposed celiotomy boundary where the linea alba is widest, which will help with piercing the linea alba directly on the midline without injuring the neighboring rectus abdominal muscles and improves the odds of accurately stabbing on the midline. A stab that is caudal to the umbilicus can make it difficult to evenly divide the narrow linea alba and is more likely to be paramedian through the rectus abdominal muscle. When enlarged or dilated visceral structures are expected to be directly below the linea alba (eg, the dilated stomach of a dog with gastric dilatation-volvulus), the linea alba can be carefully incised incrementally until the peritoneum is exposed to avoid injuring the underlying viscera.
Different tools are available for use when making the incision. Sharp straight Mayo scissors can be used to avoid cutting a curvilinear or paramedian incision through the rectilinear linea alba. As compared with the thicker, more rigid adjacent rectus muscle, the thinner, more elastic linea alba can be stabilized and creased with a straight instrument. This technique will only work if the initial stab incision is made on the midline. When a scalpel is used, a groove director or thumb forceps can help guide the incision on the linea alba midline. A groove director channel guards against accidental incision beneath the linea alba. An electrosurgical wand can also be used and, in the author’s experience, does not appear to impede healing and does not increase wound complication rates, including incisional herniation. A decision on which tool to use should be made before beginning the procedure.
Benefits of Midline Linea Alba Incision Versus Paramedian Incision
Subcutaneous vascular structures are typically parallel on either side of the ventral abdominal midline and rarely cross to the opposite side. There is less subcutaneous bleeding when the skin and subcutaneous tissues are divided directly midline (Figure 2).


Midline skin and superficial subcutaneous incision showing parallel superficial vasculature (A). Deeper subcutaneous incision showing the white line of the linea alba and parallel vasculature (B)
A paramedian celiotomy incision injures sensitive muscle tissue, which increases bleeding. Increased trauma may cause inflammation and pain. Incisions in fascia may cause less bleeding and discomfort because the linea alba is composed of poorly innervated and relatively avascular fascia.
The falciform ligament is a fat-filled fold of peritoneum that extends from the liver and diaphragm to the umbilical scar and is attached lateral to midline on the internal surface of the linea alba. Blood vessels run along the abdominal wall through these attachments. At the cranial extent of the ligament, more robust vessels enter on either side of the xiphisternum. An incision made directly midline in the fatty peritoneal fold is less likely to inadvertently damage these vessels. When additional exposure is unnecessary, the falciform ligament may be divided on the midline to avoid these vessels altogether. To improve exposure during full abdominal exploration, the falciform ligament can be excised by pulling each sleeve of the peritoneal fold from its respective abdominal attachment and separating the attachments while maintaining hemostasis. More robust cranial xiphisternal vessels should be ligated or electrocoagulated.
If the celiotomy incision is midline, suture closure will engage all fascial components of the abdominal wall with a direct needle pass. Minimal muscle should be incorporated in the sutured abdominal wall closure, which should reduce postoperative patient discomfort. Celiotomies not on midline rarely cause significant complications and can heal quickly if closed properly.
Step-by-Step: Identifying the Linea Alba & Avoiding Paramedian Incisions During Midline Celiotomy
What You Will Need
Straight Mayo scissors
Adson-Brown or Adson thumb forceps
#10 or #15 blade and handle
Groove director (optional)
Electrosurgical wand (optional)
Step 1
Position the patient in dorsal recumbency squarely symmetrical on the operating table. Palpate the umbilical scar and xiphoid cartilage, and line up on the midline with the skin raphe between the mammary chains.
Author Insight
The patient should not be rotated on its longitudinal axis, as loose skin on dogs and cats can be twisted out of neutral position during positioning. Improperly positioning the patient commonly causes incisions to be off midline and can cause failure to identify the linea alba.
Step 2
Use a scalpel blade or electrotomy to dissect cleanly and atraumatically through the subcutaneous tissues of the proposed celiotomy approach. Avoid blunt dissection, and achieve hemostasis throughout. Sharply dissect the paramedian subcutaneous tissue directly to the fascia, control any hemorrhage, then sharply dissect directly between the subcutaneous fat layer and fascia. No hemorrhage should be expected during this deeper sharp dissection, and no fat should shroud the fascia.
Author Insight
Poor hemostasis during skin and subcutaneous separation can cause deeper tissues to stain and make distinguishing subcutaneous from fascial layers difficult. Wiping tissue with gauze sponges or fingers can result in further staining and cause the white-colored linea alba to blend in with more uniformly stained-pink adjacent tissue.
Palpating the linea alba when the shiny, light-colored fascial layer is exposed should not be attempted. Although the umbilical scar can be routinely felt as a solid landmark, the remaining linea alba feels like an indistinct depression and can rarely be distinguished from the surrounding fascia by digital palpation. Rubbing, especially if there is residual blood in the field, may further prevent the surgeon from spotting the linea alba.
For exposure of the caudal abdomen in male dogs, the skin and subcutaneous incisions should run paramedian to avoid injuring the prepuce or penis.
Step 3
Assess the direction of the exposed fibers of the ventral abdominal fascia to help identify the location of the linea alba. If the linea alba cannot be isolated and the incision is believed to be paramedian, carefully lift the cut edge of the subcutaneous tissue on the side suspected of housing the linea alba. Carefully and sharply dissect between the subcutaneous tissue and fascia until the linea alba is identified. Avoid blunt dissection through the subcutaneous fat, as this will leave a fringe of fatty tissue overlay that obscures identification.
Author Insight
Ventral abdominal fascia fibers typically angle caudomedially and join at the linea alba and may be obvious in some animals. Increased skill and experience in identifying the linea alba can make cleaning (ie, undermining) subcutaneous tissue off the midline seldom necessary. Excessive undermining increases dead space and the potential for seromas, causes more hemorrhage, and is likely to increase tissue trauma, inflammation, and pain.
Step 4
Stab on the midline and use a lift-and-push cut maneuver with scissors to expand the incision (see Step 6). If possible, avoid stabbing through the region of a previous celiotomy scar, as organs are often closely adhered to the deep side of the linea alba scar and there is risk for accidental organ damage. Elevate the linea alba with Adson or Adson-Brown thumb forceps to minimize the risk for trauma to underlying organs during the stab incision. Turn the scalpel’s cutting blade upward and create a controlled stab with the blade held at a 45° angle.

Proper scalpel stab incision at a 45° angle with the blade pointing away from viscera
Author Insight
Before the initial stab approach is extended, inserting an index finger through the incision can help check for adhesions, falciform ligament attachments, or other structures adhered to the proposed fascial incision line.
Step 5
Ensure that the stab incision passes fully through the linea alba into the peritoneal cavity. Pass a blunt instrument through the stab incision. If the instrument does not readily pass through the incision, extend the external fascial incision several centimeters, pick up the exposed internal rectus sheath with thumb forceps, and carefully incise into the peritoneal cavity.
Author Insight
Extending the incision can be difficult if the stab incision is incomplete; the instrument will not slide under the fascia and will get caught in the rectus sheath, which will inhibit further fascial incising.
Step 6
Based on the incision tool chosen prior to surgery, follow the appropriate guideline below.
Using Straight Mayo Scissors
Hold the scissors firmly against the linea alba to follow the inner crease (ie, furrow). While holding the stab incision site away from viscera, open the scissors slightly and insert the blunt-tipped blade of the scissors fully through and against the inner surface of the linea alba. After the blade is inserted, lift and lever the blade against the inner linea alba. Use the index finger of the hand opposite the one holding the scissors to lift the hinge area of the scissors, seating the cutting scissor blade against the furrow under the linea alba. Keep the tip of the inserted cutting blade close to the abdominal wall to protect against visceral injury. Using a push-cut technique, slide the scissors (still only slightly open) along the linea alba. Keep the blade fully inserted and firmly seated to accurately guide the scissors’ cut.
Author Insight
If the tissue snags and prevents easy sliding during the push-cut technique, use a typical scissors cut but do not cut past the midpoint of the blade length before advancing the scissors against the hinge for the next cut. The cut can fall from the midline and into the muscle if the blade loses contact with the guiding furrow.

Straight Mayo scissors held against the linea alba before the push-cut incision
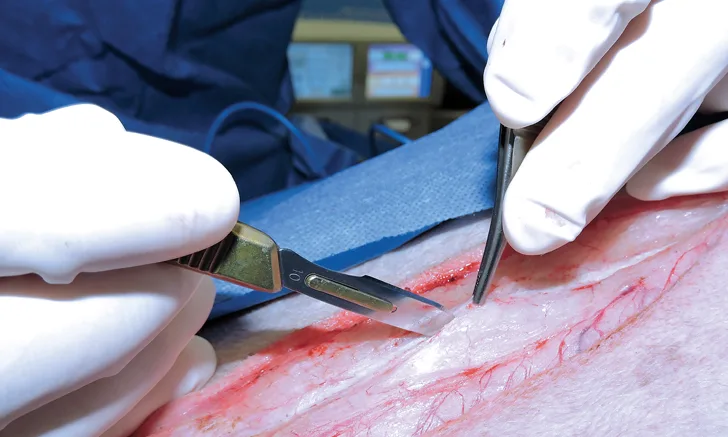
Using a Scalpel
Holding the thumb forceps tips partially closed with the nondominant hand, insert them 1 cm or more into the stab incision directly under and in line with the linea alba. Lift the forceps tips and keep them elevated while making the sharp incision. When incising, hold a #10 scalpel at a 30° to 45° angle with the dominant hand, and insert the cutting blade tip between the tips of the thumb forceps. Switch hands with the one holding the scalpel and thumb forceps and continue the linea alba incision in the opposite direction. As a unit, slide the thumb forceps and scalpel blade along the linea alba.
Alternately, insert the blunt end of a groove director with the channel pointed up through the stab incision for several centimeters. While holding the butterfly end of the groove director and lifting the instrument against the linea alba furrow, slide the groove director and scalpel blade together as a unit to continue the incision.
Author Insight
When the linea alba is cut on the midline, the incised edges will not have exposed muscle. If muscle is exposed on one side of the fascial incision, deviate the direction of the cut slowly to the opposite side until no muscle is exposed.


Scalpel blade moving within the groove of a director (A). Adson-Brown thumb forceps lifting the linea alba while a scalpel blade incises it (B)
Using an Electrosurgical Wand
After the stab incision, fully insert an index finger underneath and along the linea alba and lift it from the abdominal viscera. With the electro-surgical wand on cutting mode, begin cutting the distinct white linea alba line while carefully observing the edges of the wall incision behind the electrode. Use the same method as when using a scalpel to keep the incision from straying paramedian into adjacent rectus abdominal muscle.
Author Insight
The surgeon’s finger under the linea alba will not be injured during electrosurgical incision (ie, electrotomy) if the patient is properly grounded and the surgeon’s glove has not been perforated. Tissue in immediate contact with the electrode may become hot to the touch if the incision does not proceed at a proper rate. Temporarily moving the electrode away from the tissue will allow tissue to cool and the electrotomy can proceed.


Muscle tissue is not exposed, which indicates that the cut is directly on the linea alba (A). Muscle is exposed only on one side, which indicates that the incision is beginning to stray to that side (B).