Hyperglycemia: A Complete Guide for Dogs & Cats
Thomas Schermerhorn, VMD, DACVIM (SAIM), Kansas State University

Hyperglycemia is defined as an increase in blood glucose levels above the physiologic range for a given species. Hyperglycemia may be physiologic or pathologic and is always secondary to a disorder that disrupts one or more of the homeostatic mechanisms that maintain euglycemia.
Background & Pathophysiology
Glucose is a principal fuel metabolized to produce adenosine triphosphate for use in cellular-energy–requiring processes and is vital for normal cell function. Homeostatic mechanisms maintain blood glucose levels within narrow physiologic limits (ie, euglycemia).1 Glucose ranges in dogs and cats vary slightly but generally measure ≈90 mg/dL.2
Glucose homeostasis is a balance between glucose appearing in and disappearing from the blood (Figure). Normoglycemia is maintained by the complex interactions of a group of hormones that exert hyperglycemic or hypoglycemic actions by altering the metabolic pathways that produce or consume glucose.3 Insulin, produced by β cells in the pancreatic islets, is the most important hormone for maintaining glucose homeostasis. Insulin secretion is precisely regulated by glucose. In circulation, it exerts potent hypoglycemic actions by promoting cellular uptake of glucose, stimulating hepatic glycogenesis, and suppressing hepatic gluconeogenesis.4 Several hormones that promote hyperglycemia oppose insulin’s hypoglycemic actions. Glucagon, also of pancreatic islet origin, activates hepatic glycogenolysis and gluconeogenesis pathways that increase net glucose production by the liver.3 Thyroid hormones exert a hyperglycemic action, especially when secreted in excess, as in hyperthyroidism.3 Adrenal catecholamines (eg, epinephrine, norepinephrine),5 cortisol,6 and growth hormone7 also antagonize insulin action. Glucagon, growth hormone, catecholamines, and cortisol are collectively called “counterregulatory hormones” to reflect their functions as insulin antagonists. These hormones are the physiologic foundation of hyperglycemia that develops as part of the “fight-or-flight” response, but individual hormones play roles in various disorders that have insulin resistance as a common pathology.8
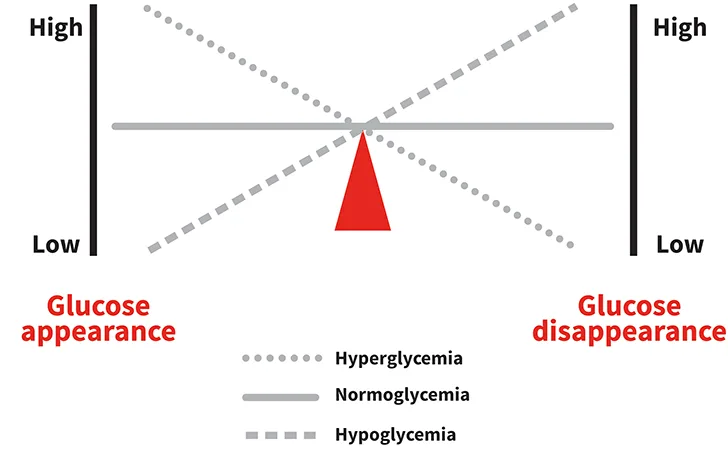
The relative rates of glucose appearance into and disappearance from the blood affects glycemic status. Normoglycemia (solid line) is maintained when the rates of appearance and disappearance are balanced. Hyperglycemia (dotted line) results when the rate of appearance exceeds the rate of disappearance, and hypoglycemia (dashed line) occurs when disappearance exceeds appearance.
Mechanisms of Action
Homeostatic mechanisms responsible for normoglycemia maintenance are robust and persistent. Hyperglycemia does not occur when physiologic pathways are intact; instead, it appears when glucose enters the blood faster than it can be removed (Figure). Pathologic hyperglycemia develops when physiologic mechanisms that suppress glucose are lacking (as in hypoinsulinemic states) or attenuated (as in insulin-resistant states).9 Once hyperglycemia is established, chronic elevation of blood glucose levels exacerbates the existing defects in pathways for β-cell secretion and insulin action in target tissue, a phenomenon termed glucose toxicity.
Hypoinsulinemia
Hypoinsulinemia is an absolute or a relative decrease in blood insulin levels. Absolute hypoinsulinemia is caused by β cell loss, whereas relative hypoinsulinemia occurs when insulin is unable to mount an appropriate response to increased blood glucose levels. Hypoinsulinemia is a hallmark of advanced diabetes mellitus in dogs and cats, regardless of the underlying pathology.10
Insulin Resistance
Insulin resistance is a metabolic state in which target tissues resist the hypoglycemic actions of insulin (ie, decreased insulin sensitivity). Insulin resistance interferes with insulin-mediated cell signaling and reduces glucose uptake in peripheral tissues, especially skeletal muscles and adipose tissue.4 With reduced insulin effects at the cellular level, the pancreas must produce more insulin. This insulin resistance results in hyperinsulinemia, an early feature of hyperglycemia (ie, hyperinsulinemic hyperglycemia). However, patients that are chronically insulin-resistant may develop β-cell failure and hypoinsulinemia (ie, hypoinsulinemic hyperglycemia).4
Hyperglycemia produces pathology by inducing hyperosmolality (which underlies the commonly observed clinical signs) and producing advanced glycation end products (AGEs), a process that is associated with end-organ damage in vascular and neuronal cells.11
Pathology
Glucose is a serum osmole but contributes little (3-5 mOsm/L) to the total serum osmolality in normoglycemic dogs and cats.12,13 The osmolar contribution of glucose parallels the magnitude of hyperglycemia and can be substantial in cases of severe hyperglycemia (eg, >50 mOsm/L when glucose exceeds 1000 mg/dL).12 Complications of hyperosmolality observed with severe hyperglycemia include vomiting, neurologic impairment, seizures, and coma.13 The onset of hyperosmolality initially triggers corrective physiologic responses, including thirst and reduced renal excretion of free water.14 Chronic hyperosmolality induces additional adaptations, including expanded blood volume and altered water metabolism.
Hyperglycemia also permanently alters cellular and serum proteins through a nonenzymatic glycation reaction that produces a series of AGEs.11 Some glycated proteins (eg, hemoglobin A1c and fructosamine) serve as clinical biomarkers that reflect average blood glucose levels over time.15 Other AGE proteins interact with specialized receptors of AGEs that are expressed by vascular and neuronal tissues, a reaction that is implicated in long-term diabetes complications, such as microangiopathy and neuropathy.11
Common Conditions Associated with Hyperglycemia
Numerous causes of hyperglycemia have been identified in dogs and cats (see Causes of Hyperglycemia). Several frequently encountered endocrine causes illustrate how pathologic disorders disrupt normal homeostatic mechanisms to cause this disorder.
Causes of Hyperglycemia2
Common Causes2*
Physiologic (ie, stress hyperglycemia) hyperglycemia (cats, dogs)
Diabetes mellitus (cats, dogs)
Hyperadrenocorticism (dogs)
Acromegaly (cats)
Acute pancreatitis (cats, dogs)
Drug- and toxin-induced hyperglycemia (cats, dogs)
Glucocorticoids
Progestogens
α2-receptor agonists
β blockers
Glucose-containing crystalloid fluid
Parenteral feeding solution
Ethylene glycol ingestion
Uncommon & Miscellaneous Causes
Postprandial hyperglycemia
Pancreatic neoplasia
Diestrus (dogs)
Critical illness or sepsis
Pheochromocytoma
Hyperthyroidism (cats)
Head injury/trauma
*Although these etiologies are diverse, common mechanisms underlie the development of hyperglycemia. Hyperglycemia in these conditions is caused by either a pathophysiologic disturbance in the ability to produce/secrete normal amounts of insulin or, more commonly, induction of insulin resistance. For some disorders (eg, pancreatitis), both mechanisms may contribute to hyperglycemia.
Diabetes Mellitus
Diabetes mellitus (DM) is the most frequently encountered and clinically significant hyperglycemic disorder in small animals. Hyperglycemia in DM arises from the combined influences of hypoinsulinemia and insulin resistance. However, the proportional contribution of each mechanism may vary, depending on underlying diabetes pathology or even the stage of disease. Hyperglycemia in humans with type 1 diabetes is caused by severe hypoinsulinemia that develops as a result of autoimmune-mediated destruction of β cells.16 Likewise, marked hypoinsulinemia is a typical finding in canine DM, which shares certain pathogenic features with human type 1 diabetes. In humans, an islet defect causes disordered glucose sensing and an abnormal insulin secretion pattern in response to a glucose challenge.16 Affected humans retain the ability to make and secrete insulin, but the quantity and timing of insulin release is insufficient to maintain euglycemia, and hyperglycemia develops.16 Islet defects are not well described in canine DM and, if present, occur early in the development of DM and are not recognized clinically. In cats with overt DM due to insulinopenia, the early role of abnormal insulin secretion (the consequence of an islet defect) is not appreciated due to profound islet loss. However, the presence of an islet defect is suggested when islet mass is adequate but there is evidence for impaired glucose tolerance. For example, an islet defect is suggested by the abnormal glycemic response to a glucose challenge in obese cats at risk for DM and the abnormal glucose tolerance documented in cats that have entered diabetic remission.17 These cats are normoglycemic and have no requirement for exogenous insulin.17 Insulin resistance is a major pathologic feature of type 2 diabetes in humans, which may contribute to islet exhaustion and, eventually, hypoinsulinemia.16 Insulin resistance is not a major feature of uncomplicated canine DM but seems to play a role in pathogenesis and progression of feline DM.18
Catecholamine & Cortisol Excess
Conditions associated with elevated concentrations of catecholamines and/or cortisol produce hyperglycemia by inducing insulin resistance. Catecholamines contribute to the phenomenon of stress hyperglycemia, which serves a physiologic function and is frequently encountered in veterinary patients.5,19 The stress response is transient and typically results in mild to moderate hyperglycemia; severe hyperglycemia can occur but is uncommon. Excessive production and secretion of norepinephrine by neuroendocrine paraganglioma, as is seen in adrenal medullary tumors (pheochromocytoma), can produce hyperglycemia in ≈25% of affected dogs.20
Hypercortisolemia caused by canine hyperadrenocorticism can cause persistent hyperglycemia of varying severity via several mechanisms, including inhibition of insulin secretion and exacerbation of peripheral insulin resistance.21 Hyperglycemia due to insulin resistance can resolve when hypercortisolemia is addressed, but persistent severe insulin resistance can lead to β cell exhaustion and hypoinsulinemia that results in permanent DM.21
Growth Hormone Excess
Growth hormone (GH), or somatotropin, antagonizes insulin action and, in excess, induces severe insulin resistance. The best example in companion animals is feline acromegaly, which is caused by a functional GH-secreting pituitary adenoma. Cats with acromegaly are usually initially presented for signs related to GH excess, including glucose intolerance, insulin resistance, or, frequently, overt DM.22 In addition to commonly reported anatomic changes that accompany acromegaly, large pituitary tumors may produce neurologic signs through compression and damage to local brain structures.22
History
Patient history will vary depending on the underlying cause of hyperglycemia. DM is the most frequently encountered disorder associated with clinically significant hyperglycemia. Patients may have a subtle history that includes weight loss, often despite maintaining a normal appetite, along with increased water consumption and changes in urination habits. Patients with complicated diabetes may appear to be ill and exhibit lethargy, diminished appetite, reduced water consumption, or vomiting.2
Dogs with hyperadrenocorticism typically demonstrate profound polydipsia and polyuria secondary to hypercortisolemia, so any additive effects of hyperglycemia may go unnoticed in this setting. In some cases, the development of polydipsia or polyuria in a dog with well-controlled hyperadrenocorticism signals the onset of diabetes.21
Cats with acromegaly are often presented with uncontrolled DM. They show typical signs of DM but uniquely display persistent hyperglycemia despite provision of high doses of insulin (>2.2 U/kg/dose). It is only after other signs are recognized (eg, increased body mass, organomegaly, changes in facial structure) that acromegaly is suspected.22
Clinical Signs
The primary clinical signs of hyperglycemia are polyuria and polydipsia.2,9 These signs are most obvious with the onset of moderate to severe hyperglycemia, specifically when blood glucose levels begin to exceed the ability of the proximal tubules to reclaim filtered glucose. Glucose is freely filtered at the glomerulus, but avid reabsorption in the proximal tubules ensures that normal urine does not contain glucose. Glucosuria occurs when the amount of filtered glucose exceeds the capacity of the proximal tubules to reclaim glucose from filtrate. The renal threshold for glucose is exceeded when serum glucose levels range from >180 to 200 mg/dL in dogs and >250 to 280 mg/dL in cats.2 Polyuria and polydipsia are interrelated and develop as a result of glucose-mediated plasma hyperosmolality (which stimulates thirst and drinking behavior) and glucose-mediated osmotic diuresis (which increases the volume of urine and frequency of urination).23
Diagnosis
Hyperglycemia is diagnosed using any of several widely available laboratory methods. In most clinical situations, glucose is measured as part of most routine serum chemistry profiles but can also be measured using other methods, such as a portable glucometer or interstitial glucose monitor. Mild hyperglycemia in the absence of clinical suspicion of a hyperglycemic disorder may be transient physiologic hyperglycemia and should be re-evaluated; persistent hyperglycemia, even if relatively mild, warrants a diagnostic investigation. DM is a likely diagnosis when hyperglycemia is the sole or primary finding and clinical signs are present. However, careful evaluation is necessary to avoid DM misdiagnosis in patients presented under circumstances that might induce stress hyperglycemia (eg, severe illness, fear, anxiety), which is frequent in cats and can be marked in some patients. In rare circumstances, it may be challenging to confirm a DM diagnosis in a patient with hyperglycemia due to illness or stress. Fasting hyperglycemia or hyperglycemia that persists over multiple sampling periods or marked glucose elevation (>250 mg/dL) is suggestive of DM rather than a stress response. Although glucosuria is not essential for a diagnosis of DM, most dogs and cats have glucosuria at the time of diagnosis. Glucosuria may occur secondary to marked stress hyperglycemia in some cases and is present without concurrent hyperglycemia with conditions associated with renal tubule dysfunction (eg, primary renal glucosuria, Fanconi’s syndrome, acute renal tubular injury).24
Treatment & Management
Principal management of hyperglycemia aims to address the underlying cause. Hyperglycemia caused by insulin resistance may be ameliorated as the associated condition resolves, endocrine pancreatic function (eg, glucose-sensing, insulin secretion) normalizes, and an appropriate insulin response can be mounted. For example, hyperglycemic humans with obesity-associated insulin resistance may return to normoglycemia after weight loss. Hyperglycemia associated with glucocorticoid excess resolves when hyperadrenocorticism is addressed if β cell function is normal. Likewise, although hyperglycemia is an infrequent finding with functional canine pheochromocytoma, normoglycemia is expected to be restored after successful adrenalectomy. The insulin resistance that accompanies feline acromegaly is severe and often only fully resolves with appropriate therapy that effectively addresses excessive growth hormone.
Hyperglycemia caused by hypoinsulinemia is treated with insulin replacement. Most patients requiring insulin replacement have permanent DM, although the diabetic state can resolve under some circumstances. For example, severe pancreatitis may be accompanied by hyperglycemia, which, if severe enough, warrants use of insulin to restore euglycemia. Hyperglycemia in this setting is due to the combined effects of insulin resistance (secondary to marked inflammation) and hypoinsulinemia (secondary to islet cell injury or loss). In some cases of pancreatitis-associated DM, the need for exogenous insulin decreases and eventually resolves with resolution of pancreatitis.
Prognosis & Clinical Follow-Up
The pathologic consequences of untreated chronic hyperglycemia are similar regardless of the underlying cause. Risk for complications increases with the duration and magnitude of hyperglycemia. Microvascular injury caused by chronic hyperglycemia causes the common diabetic complications in humans (eg, retinopathy, nephropathy). Hyperglycemia also has a role in cataract formation in dogs and diabetic neuropathy in dogs and cats, as well as in humans.
Hyperglycemia is a common clinical problem in dogs and cats. The prognosis is difficult to determine because it depends on whether the underlying cause can be effectively controlled. DM in dogs and cats carries a guarded prognosis, depending on the establishment of an effective control protocol. Canine hyperadrenocorticism has a variable prognosis, depending on the initiating pathology (ie, pituitary, adrenal), but prognosis for return to euglycemia is good if hypercortisolemia is effectively controlled. Hyperglycemia associated with feline acromegaly carries a poor prognosis, primarily because diabetes control is difficult, options for treatment of growth hormone excess and pituitary adenoma are limited, and cats are often presented with advanced disease.