Hyperaldosteronism in Cats
You have asked…I have never seen a case of hyperaldosteronism. How would I recognize, diagnose, and treat it in cats? The expert says…
Aldosteronoma, a tumor of the zona glomerulosa of the adrenal cortex, produces and secretes supraphysiologic amounts of the mineralocorticoid aldosterone, which can cause hyperaldosteronism and clinical signs related to increased hormone production. In cats, aldosteronomas are fairly evenly distributed as either adenomas or adenocarcinomas.1 Similar clinical signs can occur with idiopathic hyperplasia of the zona glomerulosa, although histologic features do not predict tumor functionality.1,2
Clinical Pathology
Excessive aldosterone production causes increased sodium reabsorption and potassium excretion. Hypokalemia can result in smooth and skeletal muscle dysfunction and damage; many cats with hypokalemic myopathy exhibit varying degrees of muscular weakness, ranging from mild limb weakness to ventral cervical flexion and impaired ability to ambulate.1,2
In addition, hyperaldosteronism-associated sodium retention can cause systemic hypertension, which results in retinal bleeding and visual impairment. Chronic hypertension can also cause myocardial hypertrophy, clinical cardiac enlargement, murmurs, and eventually cardiac dysfunction. Renal dysfunction can occur because of a combination of factors, ranging from separate intrinsic renal disease to complications resulting from hypertension, rhabdomyolysis, and hypokalemic nephropathy.1-4
Medical Workup
Patients should have a complete medical evaluation, including abdominal and thoracic imaging, urinalysis, and serum biochemical analysis.
Imaging
Abdominal ultrasonography and MRI can be used to detect an adrenal tumor in cats with primary hyperaldosteronism (Figures 1 and 2, below), but neither imaging modality can distinguish between the various adrenal tumor types (ie, adenocarcinoma, pheochromocytoma, aldosteronoma).5 Thoracic radiography is useful in detecting metastatic lesions associated with adenocarcinoma.1
Figure 1 (right). Left-sided adrenal tumor seen on abdominal ultrasound: The mass measures approximately 2 cm in diameter and is seen adjacent to the posterior vena cava. The Doppler blood flow study, as shown above the mass, has no evidence of vascular invasion. The histopathologic diagnosis was adrenocortical adenoma. (view larger image)
Figure 2 (left). An MRI study showing an adrenal mass at the cranial pole of the left kidney: The urinary bladder is distended with urine containing the contrast medium. Both kidneys are clearly shown, as is the left adrenal mass lying just cranial to the left kidney. The adrenal tumor lies adjacent to the posterior vena cava, showing no signs of vascular wall invasion. (view larger image)
Laboratory Study
The complete serum biochemical profile should include BUN, serum creatinine, and serum sodium and potassium concentrations. The serum sodium is usually normal notwithstanding the increase in total body sodium. (Systemic hypertension can also cause increased cardiac afterload and left ventricular failure, but heart failure rarely develops in this clinical situation.) Excessive renal potassium excretion causes hypokalemia and marked depletion of total body potassium stores. Serum potassium values of less than 3.0 mEq/L may have adverse effects on the skeletal and cardiac muscles.
Clinically, marked hypokalemia can cause severe skeletal muscle weakness, rhabdomyolysis, and abnormalities in cardiac excitation and conduction.7,8 Because severe hypokalemic myopathy can cause severe rhabdomyolysis, the serum creatine kinase concentration may be markedly elevated. Any myoglobinuria can be tubulotoxic, thereby compromising renal function and causing increased BUN and serum creatinine concentrations.
Treatment & Prognosis
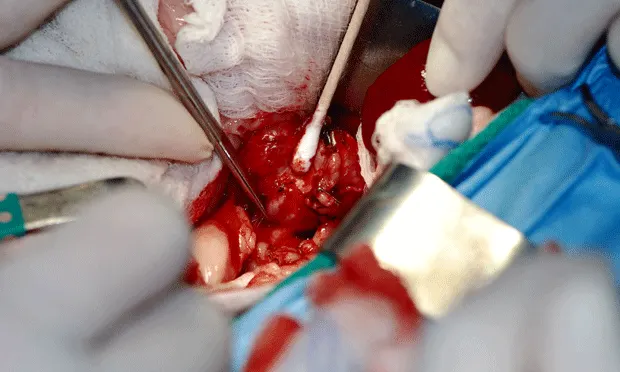
Surgery is the preferred definitive treatment for aldosterone-secreting tumors (Figure 3, right), whereas oral spironolactone, potassium gluconate, and amlodipine together represent the preferred medical approach for chronic adrenal hyperplasia. This approach also can be used as palliative treatment for tumors when surgery is not possible.
Figure 3. A left-sided aldosteronoma being dissected at surgery: The tumor is being carefully dissected with a cotton-tipped applicator. Two blood vessels have been cut and ligated using a suture ligature on one and a surgical staple on the other. Extreme care must be taken to avoid inadvertent cutting of the posterior vena cava, aorta, and renal blood vessels.
Hypokalemia (ie, potassium <3.0 mEq/L) should be treated with slow constant-rate IV infusion of a potassium chloride solution diluted in 0.45% sodium chloride. The usual therapeutic rate of administration is 0.5 mEq/kg/hr, but when the serum potassium concentration is <2.5 mEq/L, a larger dose of 1.0 to 1.5 mEq/kg/hr might be indicated, along with simultaneous electrocardiographic monitoring.7,8
Potassium supplementation using potassium gluconate tablets or powder can be administered at 2 mEq/4.5 kg PO Q 12 H. Spironolactone, a potassium-sparing agent, can be administered at 2 to 4 mg/kg PO Q 24 H. This drug blocks the effects of aldosterone at the renal distal tubule.
Cats with blood pressure readings exceeding 180 mm Hg should be treated with a calcium-channel blocker, such as amlodipine at 0.625 to 1.25 mg PO Q 24 H.
The prognosis is favorable for adrenocortical hyperplasia and when the pathology of an adrenal mass is confirmed to be benign.
The Role of Plasma Aldosterone
The clinical signs of hyperaldosteronism arise from the pathophysiologic effects of excessive aldosterone production. Typically, plasma aldosterone concentrations are markedly elevated when caused by a functional adrenal tumor (ie, aldosteronoma).1 However, because plasma aldosterone levels can increase in the presence of diseases that can stimulate the renin–angiotensin–aldosterone pathway, a definitive diagnosis cannot be reached without eliminating other causes of plasma aldosterone elevation and demonstrating either an adrenal mass or concurrent plasma renin activity.1
In one study of 11 cats with idiopathic adrenal hyperplasia-induced hyperaldosteronism, plasma aldosterone concentrations ranged from 240 to 940 pmol/L (normal range, 120–540 pmol/L); this overlap between normal and abnormal values is not uncommon in cats with tumor-free disease.2
A recent study examined aldosterone responses to varying cosyntropin doses in healthy cats; control values ranged from 57 to 119 pmol/L, whereas postcosyntropin values ranged from 99 to 341 pmol/L.6
BUN = blood urea nitrogen, MRI = magnetic resonance imaging
For related articles, see the following:Feline HypertensionMeasuring Blood Pressure
MICHAEL SCHAER, DVM, Diplomate ACVIM & ACVECC, is a professor of small animal medicine in the department of small animal clinical sciences as well as special assistant to the dean of the University of Florida College of Veterinary Medicine. In addition to be selected several times as Teacher of the Year, Dr. Schaer has received numerous awards for his clinical research in small animal internal medicine, endocrinology, and emergency and critical care medicine. Dr. Schaer is the author of various textbooks, most notably Clinical Medicine of the Dog and Cat, and is internationally recognized for his contributions in scientific publications and continuing education meetings.