How to Place an Esophagostomy Tube
Jim Wohl, DVM, Auburn University
Nutritional intervention is instrumental to supportive care for most critically ill patients. These patients have a greater protein requirement due to increased consumption of structural proteins as a source of energy.1,2 Malnourished or otherwise undernourished animals are at increased risk for immunosuppression, hormonal imbalance, infection, and aspiration pneumonia.3
The Critical Difference
Through our increased understanding of the consequences of malnutrition in the critically ill, we have realized that nutritional intervention can be a life-saving supportive care measure. As we develop more sophisticated techniques and therapies for specific diseases, nutritional support (or lack thereof) often becomes the determining factor in the outcome of critical illness.
Procedure Pearl
Esophagostomy tubes have replaced pharyngostomy tubes in veterinary medicine; they are well-tolerated, economical, and not likely to cause gagging or airway obstruction.
How Much Is Enough?
The goals of nutritional therapy are to provide adequate energy, minimize breakdown of structural proteins, and provide the essential nutrients required for metabolic processes-many commercial diets and recipes are available that provide these nutrients. Thus, when a nutritionally complete diet is used, the only remaining concern is to ensure proper dosage of calories. Two well-known formulas, based on the resting energy requirement, can be used to calculate caloric needs:
Resting energy requirement = 30(body weight in kg) + 70OR30(body weight in kg)<sup0.75sup>
Why the GI Route?
Meeting the energy requirements of critically ill patients usually provides a foundation of support for therapy of the underlying disease. In animals that are unable or unwilling to ingest nutrients, nutrition should be delivered enterally whenever the gastrointestinal tract can be used. The presence of nutrients in the intestinal lumen provides the most effective means of maintaining mucosal integrity and the barrier to toxins and microbes.4 Placement of 5- to 8-French nasoesophageal or nasogastric feeding tubes is the least invasive method for providing enteral nutrition; however, feeding through small-bore tubes is labor-intensive and limits supplementation to liquid diets.
Related Article: Percutaneously Placed Gastrostomy Tubes: Prevention and Treatment
Related Article: Percutaneous Endoscopic Gastrostomy Tube Placement
Gastrostomy vs. Esophagostomy
Because of their larger size, gastrostomy tubes placed surgically or percutaneously with the aid of an endoscope allow easier feeding of gruel type diets. (Note: not all percutaneously placed gastrostomy tubes require an endoscope). In animals undergoing anesthesia, esophageal feeding tube placement is a simple and economical choice for nutritional intervention. Esophagostomy tube feedings can be as effective as gastrostomy tube feedings, and placement of esophagostomy tubes does not require endoscopy or laparotomy. Esophagostomy tubes are not likely to cause gagging or airway obstruction as has been associated with pharyngostomy tubes.5 Placement requires general anesthesia but can usually be performed in 5 minutes.
Pros & Cons
Animals with orofacial trauma are particularly well-suited for esophagostomy tubes, which can be placed after surgical repair. Larger-bore tubes (14- to 18-French) can be used depending on the animal's size. Do not use esophagostomy tubes in animals with esophageal injury or disease (e.g., megaesophagus).
Esophagostomy tubes are well tolerated in cats and dogs and can be maintained for several weeks to months.6,7 Tubes can be capped between feedings using a Christmas tree adaptor and catheter cap. The tube does not interfere with the animal's ability or desire to return to oral feeding.
Step-by-Step: How to Place an Esophagostomy Tube
Step 1
Intubate, maintain on inhalation anesthesia, and place the patient in right lateral recumbency.
Step 2
Premeasure the tube from the mid-cervical esophagus to the ninth rib, and mark it with a permanent marker. Clip and scrub the left side of the neck. The cervical esophagus lies closest to the left side. Advance curved Carmalt forceps into the mid-cervical esophagus from the oral cavity. Use the angle of the jaw and the point of the shoulder for landmarks.

Step 3
At the mid-cervical esophagus, push the curved tip of the forceps laterally so they can be palpated underneath the skin.

Step 4
Using a number 10 or 15 scalpel blade, make a stab incision through the skin only, exposing the subcutaneous tissue and muscle layers of the esophagus. Take care to avoid the jugular and maxillofacial veins when selecting the stoma site.

Procedure Pearl
Avoid placing a tube near the gastroesophageal junction-movement of the tube can cause irritation and predispose to gastroesophageal reflux.
Step 5
Exteriorize the tip of the forceps from the esophageal lumen through the skin incision.

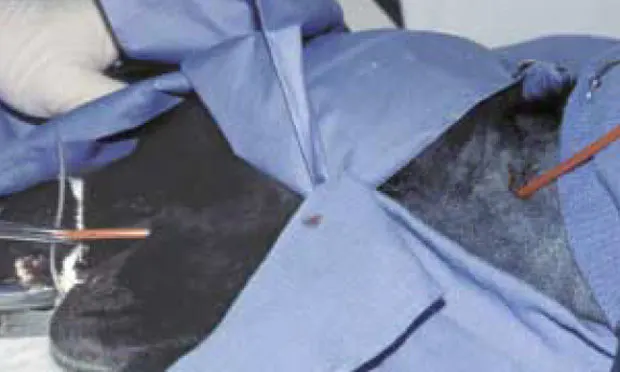
Step 6
Use the fingers of the opposite hand as shown to guide the advancing forceps. Exteriorizing the forceps in this fashion requires brief yet forceful effort. Typically, a thin white layer of esophageal mucosa must be carefully dissected off the forceps tips after penetration of the esophageal muscle layers.

Step 7
Use the forceps to clasp the distal end of the feeding tube, and draw the tube out of the oral cavity.
Procedure Pearl
Do not use esophagostomy tubes in animals with esophageal injury or disease.

Step 8
Important: Secure the distal end of the feeding tube using forceps to ensure that it remains exteriorized while the proximal tip of the tube is being withdrawn orally.

Step 9
Retroflex the proximal tip, and advance it in an aboral direction across the pharynx.
Procedure Pearl
Esophagostomy tubes should remain in place 7 to 10 days to allow fistula formation; then they can be removed and the stoma site allowed to heal.

Step 10
Maximally expose the oral cavity to facilitate pushing the tube into the esophagus. Assistance is often required for this step. Alternatively, place a lubricated stylet before the tube is redirected down the esophagus. If a stylet is being used, take extreme care to avoid withdrawing the entire tube through the esophageal stoma when redirecting the tube aborally.

Step 11
Advance the proximal tip down the esophagus. During this action, the exteriorized portion of the tube can be observed to rotate in a cranial direction. This movement indicates that the feeding tube has been placed correctly in the esophagus.

Step 12
Suture the distal portion of the tube in place using a pursestring suture and Chinese finger-trap suture pattern. Occasionally, cellulitis can occur at the tube-skin interface. For this reason, many clinicians place antibiotic ointment and gauze dressing at the incision site. Bandaging the tube in place minimizes movement at this site and decreases irritation.

Step 13
Radiographically confirm placement of the tube in the distal esophagus. Avoid placing an esophagostomy tube near the gastroesophageal junction-movement of the tube can cause irritation and predispose the patient to gastroesophageal reflux.
Step 14
Once placed, esophagostomy tubes should remain in place for 7 to 10 days to allow fistula formation. After this period, tubes can be removed and the stoma site allowed to heal by second intention.