How Local Antimicrobials Can Help Manage Periodontal Disease
Adjunct use of a locally applied antimicrobial is an option to salvage teeth with moderate to advanced periodontal disease.
An interaction between host defense mechanisms and plaque bacteria can lead to inflammation and attachment loss between the tooth and periodontal tissues (ie, gingiva, periodontal ligament, alveolar bone, cementum). Following the initial stages of gingivitis, there is attachment loss between the gingiva and the tooth and a space between the two develops. This space is known as the periodontal pocket.
If periodontal disease is untreated, deeper pockets form, bone loss results, and eventual tooth loss occurs. Periodontitis is chronic and progressive without a known cure; however, it is preventable and manageable.
Locally applied antimicrobial (LAA) agents can complement traditional scaling and root planing and can significantly improve treatment success, especially for reducing the pocket depth and regaining gingival attachment.
Clinical ImpactLAA agents (see Locally Applied Antibiotics) are slow-release products placed as a repository into a prepared periodontal pocket. These antimicrobial products contain either an antibiotic or antiseptic and are biodegradable. Although it is unrealistic to expect complete elimination of bacteria from the oral cavity, reduction in pathogenic bacterial load may contribute to the management of periodontal disease. These subgingival medications work by providing high concentrations of an antimicrobial, proven effective against periodontopathogenic bacteria, directly to diseased tissues. Local antibiotics for periodontal application contain either a tetracycline derivative or clindamycin; the only FDA-approved local antiseptic product contains chlorhexidine.
LAAs help reduce or prevent reinfection while a pocket heals. Some agents also work by physically occupying a periodontal pocket and preventing bacterial invasion and foreign body deposition while tissue heals. Local antibiotics with tetracycline derivatives display not only antimicrobial properties but anticollagenase effects as well.1,2 This property helps block tissue destruction and promotes repair. Local antibiotics with clindamycin offer the additional benefit of reducing the ability of bacteria to aggregate into large clumps.3
With use of an LAA, substantially higher doses of the drug can be dispensed in the periodontal pocket than what could be achieved by systemic dosing. For example, the first FDA-approved LAA was a nonresorbable polymer fiber saturated with tetracycline hydrochloride. Placement of this material into a periodontal pocket achieved local tetracycline levels of 1590 mg/mL. A local concentration of 30 mg/mL eliminates most pathogenic bacteria associated with periodontal disease. Despite the high doses of drug that were achieved locally, serum levels of the drug did not exceed 0.1 mg/mL.4
Indications & ContraindicationsLAAs should only be used after intraoral radiography and dental charting have been fully evaluated. Local antimicrobial products are typically considered in dogs with periodontal probing depths ≥4 mm (normal sulcus depth, 0–3 mm). In cats, the ideal depth has not been established, but because normal sulcus depth is 0 to 1 mm,5 placement of a local antibiotic can be considered in cats with pocket depths ≥2 mm.
Surgical intervention (ie, gingival flap repositioning, open-flap curettage, guided tissue regeneration) is generally required to save a tooth in dogs with periodontal pockets deeper than 6 mm, as closed root planing is ineffective in cleaning pockets.
Caretakers should be informed of the commitment involved and that not all dogs receiving LAA therapy have successful outcomes. Following initial treatment, commitment to home plaque control is key. Depending on disease severity, a follow-up procedure in 3 to 6 months should evaluate response to therapy and provide additional indicated treatment. If the client is not committed to at-home and follow-up care, the most realistic and humane treatment for the pet may be to extract the affected tooth.
Techniques & EquipmentThe most important step in improving periodontal status is professional dental cleaning with meticulous subgingival removal of plaque and calculus. Subgingival debridement includes scaling and root planing (SRP) by manual instrumentation, ultrasonic scalers, or both. SRP is standard nonsurgical treatment for periodontitis.6 If subgingival cleaning is not done, LAA application will not significantly benefit the patient. Of note, properly performed SRP is technique sensitive, and clinicians are encouraged to receive training from qualified individuals.
Once a pocket has been thoroughly cleaned and debrided, the LAA should be prepared and applied according to manufacturer recommendations. Most LAAs can be introduced into a cleaned pocket site via blunt tip cannula. In contrast, chlorhexidine gluconate in the form of a small rectangular chip (PerioChip, periochip.com) should be placed using forceps.
After placement of the LAA, treated areas should not be brushed for 1 to 2 weeks, depending on the selected product. In some cases, an oral medicated rinse should be considered to help control plaque. Application of a polymer surface barrier to the teeth can be effective in plaque management. One product (OraVet, oravet.com) has been shown to significantly reduce plaque accumulation for up to 2 weeks following professional application.7,8
AdvantagesLAAs only require one anesthetic procedure for placement, as they are biodegradable. Depending on the type selected, products generally remain active for several days to weeks. Because the agents have minimal systemic absorption, there are no known systemic adverse effects. Different methods of product placement are generally easy and quick to use. In addition, product placement requires no additional home care.
DisadvantagesGeneral anesthesia is required for full oral evaluation, preparation of periodontal pockets, and placement of LAAs. Clients should be informed of the risks involved with general anesthesia. Although local agents are fairly affordable, clients should also be informed of the costs associated with their use. Follow-up care is necessary to improve and maintain the periodontal status.
Although LAAs are considered safe, potential adverse events may include discomfort at deposition site, tooth pain, erythema, and allergic responses.4 Subgingival products should be avoided in patients with a history of hypersensitivity to the specific antimicrobial derivative. To avoid interference with tooth development in dogs younger than 1 year of age or in the embryos of pregnant bitches, products with tetracycline derivatives should not be used.
EfficacyImproved success in reducing the periodontal pocket depth is a realistic expectation when using an LAA in conjunction with SRP (compared with SRP alone).9 Therapeutic response highly depends on individual response, owner compliance in proper plaque control, and whether follow-up professional care is provided. Early detection, diagnosis, and treatment are essential for success.
LAA agents reportedly have a diversity of probing depth improvements, attachment level gains, decreased gingival bleeding scores, and improved gingival indices.9-14 Generally, it is accepted that LAA treatment with SRP should help decrease or stabilize periodontal pocket depth. Positive changes can be noted in as few as 2 weeks following treatment but would be expected to diminish over time, requiring appropriate long-term plaque management and professional follow-up visits.12
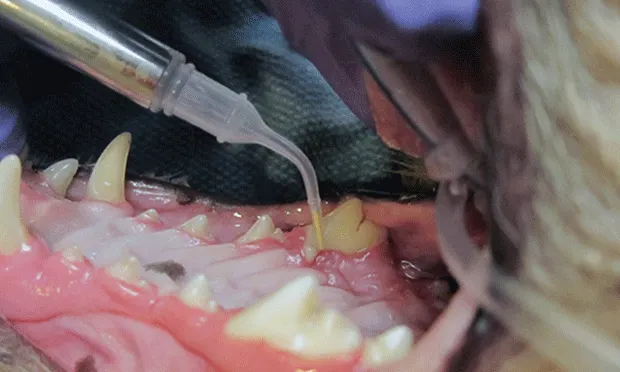
Products at a GlanceApplication of an LAA in a canine patient.
Minocycline hydrochloride (Arestin)Labeled for human use only, Arestin is a fine powder in a single-dose cartridge. The material is fairly easy to administer (Figure 1), is bioresorbable, and provides antibacterial activity against anaerobes and facultative anaerobes for 21 days.10
Clindamycin hydrochloride (Clindoral)C

lindoral is introduced to the pocket via blunt tip cannula. As it warms to body temperature, it thickens to a gelatinous consistency. This bioadhesive matrix remains in place (potentially acting as a barrier against food particles and debris) and is then bioresorbed. Clindoral must be applied to thoroughly dried tissues; this can be problematic in the oral environment.

Doxycycline (Doxirobe)The active ingredient (doxycycline) is released at high concentrations locally and shows bacteriostatic activity against pathogens associated with periodontal disease. The gel-like material is introduced with a cannula and hardens to wax-like consistency when exposed to water or oral fluids. Most practitioners can overcome the set material’s sticky nature with proper instruction and practice.
Chlorhexidine gluconate (PerioChip)PerioChip, a biodegradable, rectangular chip rounded at one end, is placed via forceps to its maximum depth into the cleaned pocket. The chip can be maneuvered further with a plastic instrument. The size of the chip limits application to periodontal pockets ≥5 mm deep.
DONALD E. BEEBE, DVM, DAVDC, is owner of Apex Dog and Cat Dentistry in Englewood, Colorado. His clinical interests include endodontics, periodontal surgery, and maxillofacial fracture repair. Dr. Beebe is a frequent local and national lecturer and teaches dental techniques at the NAVC Institute. Dr. Beebe received his DVM from University of Florida and completed a residency in dentistry and oral surgery at University of Wisconsin.
Related Article:Periodontal Health: Causes & ConsequencesPeriodontal SurgeryPain Management & Periodontal Disease
LOCAL ANTIMICROBIALS FOR PERIODONTAL DISEASE • Donald E. Beebe
References
1. Tetracyclines inhibit tissue collagenase activity. A new mechanism in the treatment of periodontal disease. Golub LM, Ramamurthy N, Gomes B, et al. J Periodontal Res 19:651-655, 1984.2. Treatment of periodontal pockets with doxycycline in beagles. Zetner K, Rothmueller G. Vet Ther 3:441-452, 2002.3. Management of periodontal disease: understanding the options. Harvey CE. Vet Clin North Am Small Anim Pract 35:819-836, 2005.4. Nonsurgical approaches for the treatment of periodontal diseases. Ryan ME. Dent Clin North Am 49:611-636, 2005.5. Veterinary Dentistry: Principles and Practice. Wiggs RB, Lobprise HB (eds)—Philadelphia: Lippincott- Raven, 1997, pp 186-231.6. Rationale for periodontal treatment. Carranza FA. In Newman MG, Takei H, Carranza F (eds): Carranza’s Clinical Periodontology, 9th ed— Philadelphia: Saunders Elsevier, 2001, pp 507-512.7. Evaluation of a barrier dental sealant in dogs. Gengler WR, Kunkle BN, Romano D, Larsen D. J Vet Dent 22:157-159, 2005.8. Evidence-based veterinary dentistry: A systematic review of homecare for prevention of periodontal disease in dogs and cats. Roudebush P, Logan E, Hale FA. J Vet Dent 22:6-15, 2005.9. Impact of local adjuncts to scaling and root planing in periodontal disease therapy: A systematic review. Bonito AJ, Lux L, Lohr KN. J Periodontol 77:1227-1236, 2005.10. Local minocycline as an adjunct to surgical therapy in moderate to severe, chronic periodontitis. Hellström MK, McClain PK, Schallhorn RG, et al. J Clin Periodontol 35:525-531, 2008.