Feline Asthma
Laura A. Nafe, DVM, MS, DACVIM (SAIM), University of Missouri
Feline asthma is a lower airway disease that affects 1% to 5% of cats,1 most commonly young to middle-aged cats.1 Although median age on diagnosis has been reported to be 4 to 5 years, most cats with asthma experience clinical signs earlier in life.1 Classified as an allergic disease, feline asthma is the result of a type-1 hypersensitivity to specific aeroallergens.2 This immune response results in cytokine release and elaboration that can ultimately cause pathologic airway changes.
Hallmark clinical features of asthma include bronchoconstriction, airway edema, airway eosinophilia, and excessive mucus production. The combination of these features can result in cough, tachypnea, and/or expiratory dyspnea.1,3 Compounding airway edema, smooth muscle bronchoconstriction, and mucus hypersecretion can result in airflow limitation, which can be at least partially reversible with bronchodilator therapy. If left untreated, chronic airway inflammation can result in irreversible airway remodeling.
Clinical Signs
Clinical signs associated with feline asthma include cough, tachypnea, open-mouth breathing, and/or respiratory distress, typically characterized by a prolonged expiratory phase of respiration and abdominal push. Some patients may have only one of these clinical signs, whereas others may have both a chronic cough and intermittent exacerbations resulting in respiratory distress with expiratory effort.3 Accordingly, clinical signs can be episodic and vary in severity, from a mild, intermittent cough to life-threatening dyspnea (ie, status asthmaticus). Pet owners may struggle to identify a true cough and may be confused with “vomiting hairballs” without production of a hairball.
Diagnosis
Definitive diagnosis of feline asthma can be challenging due to clinical features that overlap with various other cardiopulmonary conditions, including chronic bronchitis, heartworm-associated respiratory disease, and pulmonary parasitic disease. Diagnosis can be facilitated through a combination of consistent historical information, clinical signs (ie, cough and/or respiratory distress), physical examination, laboratory data (eg, CBC, serum chemistry profile, fecal flotation and analysis, urinalysis, heartworm antigen and antibody testing), imaging (eg, thoracic radiography, thoracic ultrasonography, CT, bronchoscopy, echocardiography), airway sampling, and additional diagnostic testing (eg, airway cytology) to rule out other causes of eosinophilic airway inflammation.
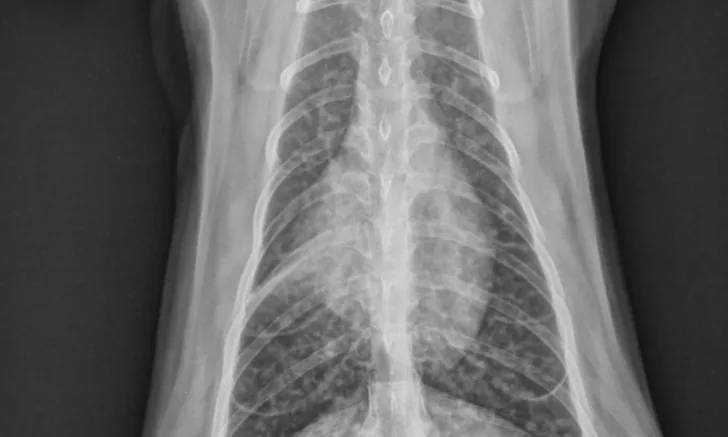
Physical examination may be normal or may reveal tachypnea, inducible cough on tracheal palpation, and/or abnormalities on thoracic auscultation (eg, increased bronchovesicular sounds, expiratory wheezes). Classic radiographic findings include a diffuse bronchial or bronchointerstitial pattern, hyperinflation due to air trapping, and/or collapse of the right middle lung lobe due to mucus plug obstruction (Figure 1).3,4 Because ≈20% of asthmatic cats have normal thoracic radiographs, asthma should remain on the differential list for any cat with respiratory distress and normal thoracic radiographs.5 In addition, a bronchial or bronchointerstitial pattern is also the predominant pulmonary pattern seen in cats with chronic bronchitis and/or heartworm-associated respiratory disease, making it challenging to differentiate these conditions from asthma via only physical examination and radiography.

Ventrodorsal thoracic radiograph of an asthmatic cat demonstrating a diffuse bronchial pattern and collapse of the right middle lung lobe, which developed secondary to mucus accumulation and resulted in atelectasis
Bronchoscopy may be used in asthmatic cats to evaluate airway structure and collect bronchoalveolar lavage fluid (BALF) for cytology, culture and susceptibility testing, and Mycoplasma spp PCR testing. Alternatively, blind bronchoalveolar lavage may also be performed in cats that show diffuse radiographic changes. Clinicians should be cautious when interpreting BALF culture and Mycoplasma spp PCR results in combination with BALF cytology results, as airways (especially the trachea) are not sterile and the presence of bacteria or Mycoplasma spp does not equate to active infection.6
Bronchoscopy findings are often nonspecific in asthmatic patients and may include excessive mucus accumulation, airway hyperemia, and/or epithelial irregularities.1 Eosinophilic airway inflammation is characteristic of but not specific to asthma (Figure 2), as parasitic disease commonly results in airway eosinophilia. Historically, eosinophilic airway inflammation has been defined as >17% eosinophils present in BALF; however, recent evidence suggests that >5% eosinophils is considered abnormal in feline BALF.7,8 Clinicians should evaluate BALF eosinophil percentage in light of clinical signs and concurrent conditions associated with eosinophilia (eg, allergic skin disease). Most asthmatic cats typically have significant BALF eosinophilia; some can have lower eosinophil and higher neutrophil numbers, particularly in chronic asthma cases. A heartworm antigen and antibody test, fecal flotation, and Baermann test should be performed in all cases. In addition, the author commonly institutes empiric antiparasitic treatment, even if results are negative.
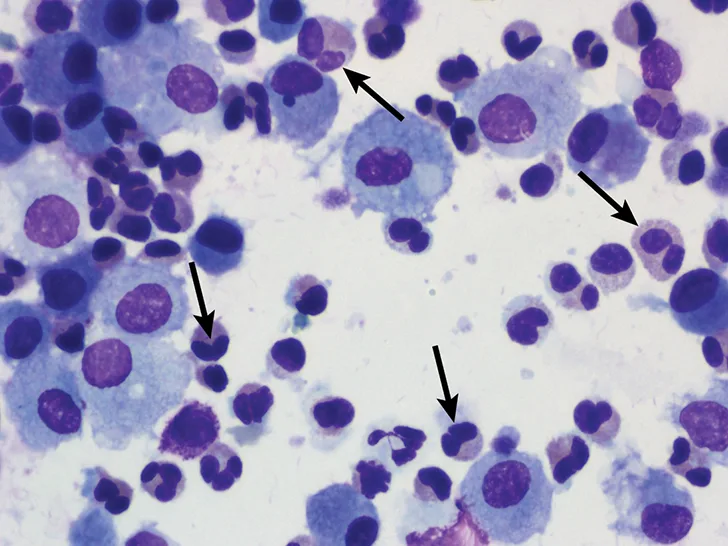
BALF cytology from a cat demonstrating a predominance of eosinophils (arrows), which is characteristic of feline asthma. Image courtesy of Dr. Susan Fielder, Oklahoma State University
Treatment & Management
Management of feline asthma consists of both acute and chronic treatment strategies. Clinicians and owners should understand that asthma is not a condition that can be cured; lifelong environmental and medical management are necessary.
Cats presented in status asthmaticus require acute management consisting of supplemental oxygen, stress reduction and minimal handling, and bronchodilator therapy (eg, inhaled albuterol [via metered dose inhaler], injectable terbutaline). In the author’s clinical experience, injectable terbutaline is preferred over inhaled albuterol in the emergency setting, as cats in respiratory distress typically may not inspire deeply enough to appropriately deliver inhaled medication to the lower airways. Identifying an expiratory respiratory pattern can be suggestive of bronchoconstriction and may lead the clinician to implement early intervention with bronchodilator therapy. Expiratory respiratory patterns are characterized by an abdominal push during exhalation. If an obvious expiratory pattern is not identified, evaluation for other causes of respiratory distress (eg, pleural effusion, congestive heart failure) should be performed prior to empiric treatment with a bronchodilator. Clinicians should evaluate patients for a heart murmur or gallop rhythm and perform cage-side thoracic ultrasonography to assess for pleural effusion and/or pulmonary edema (eg, presence of B lines). If other causes of respiratory distress are not evident on initial evaluation, intervention with a bronchodilator for possible asthma may be warranted.
Management of chronic feline asthma is aimed at reducing airway inflammation and preventing or reducing airflow-limiting bronchoconstriction.1 Reduced inflammation is best achieved by minimizing exposure to aeroallergens and environmental irritants (eg, aerosols, dust) and administration of oral glucocorticoids (eg, prednisolone). Minimizing environmental allergens is best achieved by reducing exposure to known allergens (eg, eliminating outdoor access), cleaning bedding and other surfaces in the household frequented by the cat, and using an air filter to improve air quality. Oral glucocorticoid (prednisolone) therapy should be initiated at a dose of 1-2 mg/kg/day. The dose may be tapered by 25% to 50% every 2 to 4 weeks depending on clinical response. The goal is to taper steroids to the lowest effective dose.
Inhalant Therapy
Some cats can be transitioned to receiving only inhaled steroid therapy (eg, fluticasone) to minimize the systemic adverse effects of oral glucocorticoids and maintained on inhaled glucocorticoids alone for long-term management.9 It is important to overlap the inhaled steroid with oral glucocorticoid therapy, as it is believed that inhaled glucocorticoids require ≈2 weeks to achieve full clinical effect. Although the author frequently initiates inhaled fluticasone at a dose of 110 μg every 12 hours, a study evaluating inhaled fluticasone in cats with experimentally induced asthma found that airway eosinophilia was controlled with a variety of doses, including 44 μg, 110 μg, and 220 μg, administered every 12 hours.9 The efficacy of lower-dose fluticasone has not been evaluated in cats with naturally occurring asthma. In cats with concurrent conditions in which systemic glucocorticoids are contraindicated (eg, congestive heart failure, diabetes mellitus), inhaled glucocorticoid therapy and/or oral cyclosporine may be considered.9,10
Bronchodilator Therapy
Chronic bronchodilator therapy is not necessary in all cats with asthma and is only recommended in patients that have signs associated with bronchoconstriction (eg, respiratory distress, episodic tachypnea). Inhaled racemic albuterol should not be used for chronic management of bronchoconstriction due to the proinflammatory effects of the S-enantiomer; however, racemic albuterol can be used at home by owners for rescue as needed.11 Oral terbutaline or theophylline may also be used for chronic bronchodilator therapy. Although many patients may need bronchodilator therapy initially, once airway inflammation is controlled with glucocorticoid therapy, many can be weaned off bronchodilators long-term and managed as needed. In addition, feline asthma should never be managed with bronchodilator therapy alone, as bronchodilators will not address airway inflammation, which is an integral component of controlling asthma.
Additional Therapeutic Options
Various other therapeutic drugs (ie, cyproheptadine, cetirizine, nebulized lidocaine, maropitant) have been investigated for management of experimentally induced asthma in cats12-14; although some show promise in reducing airflow limitation, none have been shown to be effective as monotherapy for management of feline asthma. As a result, these other therapeutics can be considered as adjunctive treatments along with glucocorticoids. Immunotherapy and mesenchymal stem cell therapy have shown promise as future novel therapeutics and warrant further investigation both in cats that have experimental and naturally occurring asthma.15,16
Prognosis & Prevention
Prognosis for feline asthma is typically good with prompt diagnosis and appropriate management. Status asthmaticus, however, is a potentially life-threatening manifestation of asthma in cats, especially if not recognized and treated appropriately in the emergency setting. Prevention is challenging, as it is impossible to truly prevent the onset of an allergic condition like asthma. Prevention and/or reduction of clinical signs can be achieved through avoidance of known aeroallergens.
Clinical Follow-Up & Monitoring
Follow-up evaluation is necessary for successful chronic management of cats with asthma. Clinicians should decide whether to reduce a steroid dose based on clinical signs, physical examination, thoracic radiography, and, occasionally, resolution of airway eosinophilia. Long-term management of feline asthma is aimed at lowering glucocorticoid doses to the lowest effective dose that controls clinical signs and airway inflammation. Some patients may be transitioned to inhaled glucocorticoid therapy (eg, fluticasone) using a space chamber to aid drug delivery. Patients started on bronchodilator therapy can often be tapered off once airway inflammation is controlled.
Feline asthma patients are generally responsive to treatment with a glucocorticoid ± bronchodilator. In feline respiratory patients unresponsive to standard asthma therapy, the diagnosis should be reconsidered and further diagnostics pursued.