Echocardiography in General Practice: Cardiac Abnormalities
Although proficiency in echocardiography requires training and practice, echocardiography does not necessarily have to be restricted to specialty practice. For an overview of 4 basic echocardiographic views, view our article, Echocardiography in General Practice: 4 Views to Master.
Part 2 of this series will look specifically at echocardiography for the following cardiac abnormalities:
myxomatous mitral valve disease (MMVD)
dilated cardiomyopathy (DCM)
hypertrophic cardiomyopathy (HCM)
pleural and pericardial effusions
Heart Disease Classification
Preclinical heart disease is defined as the stage of disease when a patient has evidence of cardiovascular disease. Clinical heart disease or heart failure is defined as the stage of disease when a patient has or had clinical signs attributable to their cardiovascular disease. Classification schemes that incorporate the presence and absence of signs of heart disease or heart failure with structural heart changes provide a platform for discussion of both diagnosis and treatment of common heart disease.
The classification system used for veterinary patients has been adapted from the American College of Cardiology/American Heart Association’s classification system for humans. This system describes 4 basic stages of heart disease, some of which are characterized by signs of heart failure. Patients will typically progress from one stage to the next, unless a treatment is instituted that delays or prevents this progression, or another comorbidity abbreviates the patient’s lifespan.
Classifying Stages of Heart Disease in Veterinary Patients
1. Echocardiographic Evaluation of Myxomatous Mitral Valve Disease
Myxomatous mitral valve disease (MMVD) is the most common cardiac disease in dogs. As many as 75% of dogs with congestive heart failure have mitral regurgitation due to MMVD as the underlying cause.
Cardiac auscultation is imperative in the diagnosis of mitral regurgitation. The classic mitral regurgitation murmur is systolic in timing with a point of maximal intensity over the left apex. Generally, intensity (ie, grade) of the murmur does correlate with severity, but this is not always the case. Dogs with a low-grade murmur and a clearly audible S2 are likely to have mild disease, for example, while the murmur becomes louder and S2 is obscured with more severe disease. Differential diagnoses for a murmur of mitral regurgitation include MMVD, dilated cardiomyopathy (DCM), endocarditis, and mitral valve dysplasia. Occasionally, a mid-systolic click may be auscultated with MMVD of the mitral valve before the onset of a murmur. This is thought to result from prolapse of the mitral valve and is a specific finding for mild MMVD, as there is little to no mitral regurgitation at this stage.
Thoracic radiographs are helpful to assess cardiac size when evaluating a patient for MMVD. If an abnormally large VHS is identified, echocardiography can be helpful in staging the disease and making treatment recommendations. The most important structures to evaluate are the left atrium, left ventricle, and mitral valve. Although diagnosis is relatively straightforward in dogs of a typical age and breed (eg, Cavalier King Charles spaniel or a small-breed dog aged more than 10 years) with a visualized thickened mitral valve, using advanced techniques to determine prognosis and therapy may present a challenge. Echocardiographic measurements taken during routine recheck evaluations, including left ventricular chamber dimension in diastole and systole and left atrial diameter, are used for comparison and to determine the progression of the patient’s disease.
Stage B1 Early MMVD
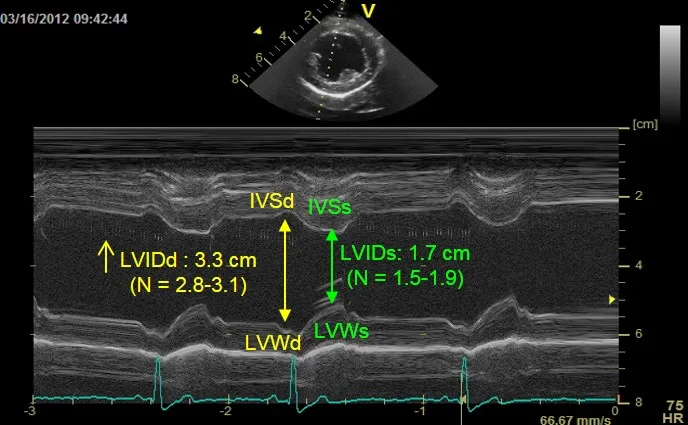
This patient was diagnosed with Stage B1 degenerative myxomatous mitral valve disease. The dog has mild left ventricular volume overload left ventricular internal dimension during diastole (LVIDd) = 3.3 cm (Range: 2.8-3.1 cm).
Stage B2 Advanced MMVD
This patient was diagnosed with Stage B2 degenerative myxomatous mitral valve disease. The patient has an obviously thickened mitral valve which prolapses into the left atrium during systole.
IVSd = interventricular septum in diastole, IVSs = interventricular septum in systole, LVIDd = left ventricular internal dimension in diastole, LVIDs = left ventricular internal dimension in systole, LVWd = left ventricular wall in diastole, LVWs = left ventricular wall in systole
2. Echocardiographic Evaluation of Dilated Cardiomyopathy
Dilated cardiomyopathy (DCM) refers to all idiopathic myocardial diseases in which myocardial (systolic) failure is the primary cardiac dysfunction.
The definitive diagnosis of DCM should be made by documenting systolic dysfunction and ruling out underlying causes of secondary myocardial failure. In a predisposed breed, such as Doberman pinscher, Irish wolfhound, Great Dane, or Newfoundland, diagnosis is often made based on echocardiographic findings. In non-predisposed breeds and in cats, an effort should be made to rule out reasonable underlying causes. Many dogs with mild to moderate DCM do not demonstrate clinical signs for years prior to presentation (ie, “clinically normal” or “preclinical”). Most dogs with DCM present for relatively acute signs of heart failure. Weakness and exercise intolerance may be noted by an astute owner, but more commonly, congestive signs are first recognized, including cough, tachypnea, dyspnea, orthopnea with left-sided congestive heart failure, and abdominal distension with right-sided congestive heart failure. Ventricular arrhythmias may cause syncope, collapse, or sudden death.
An S3 gallop is an important, but subtle, finding and may be the only abnormality identified in preclinical DCM. A soft murmur (grade I-III/VI) over the left apex due to functional mitral regurgitation is frequently auscultated. Arrhythmias may also be auscultated and may lead to pulse deficits. Arterial pulses are typically weak due to poor stroke volume. Cough, tachypnea, dyspnea, orthopnea, increased bronchovesicular sounds, and crackles may occur with left-sided congestive heart failure. Diagnosis of DCM in a typical breed can be made by using published breed standards for left ventricular systolic and diastolic diameters (see Suggested Reading).
If it is difficult to align the M-Mode cursor correctly over the 2-dimensional image, use 2-dimensional images for accurate assessment of size and function. M-Mode and 2-dimensional images are measured the same way. Diastolic measurements are made at the largest chamber size or at the beginning of the QRS complex if an electrocardiogram (ECG) is used during the echocardiogram. Systolic measurements are made at the smallest chamber size regardless of the specific point on the ECG. Systolic function can be assessed by several commonly used indices; however, these do not directly assess contractility, as all are affected by both preload and afterload. Fractional shortening (FS) is the most common index of left ventricular systolic function; it measures the fractional change in systolic and diastolic internal dimensions. FS, calculated from M-mode measurements, provides an estimate of the heart’s ability to contract.
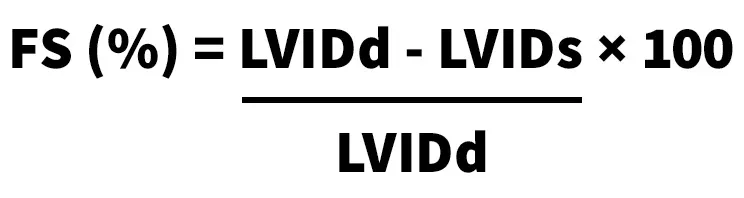
Normal FS is 25% to 45% in dogs and 30% to 55% in cats.
Of importance, FS is based on singe-dimension measurements and may not accurately reflect regional changes. In addition, this measurement is highly dependent on preload through the inclusion of LV internal dimensions in diastole (LVIDd). Although LVIDs depends on afterload, it has less relation to preload and by itself can be used as a measurement of myocardial function. Panting dogs often have excessive motion of the cardiac structures, which can lead to incorrect impressions of depressed systolic function. Clinicians must be careful not to overinterpret analysis of systolic function. If there is any doubt, a board-certified cardiologist should be asked to make the final assessment of systolic function.
Stage B1 DCM
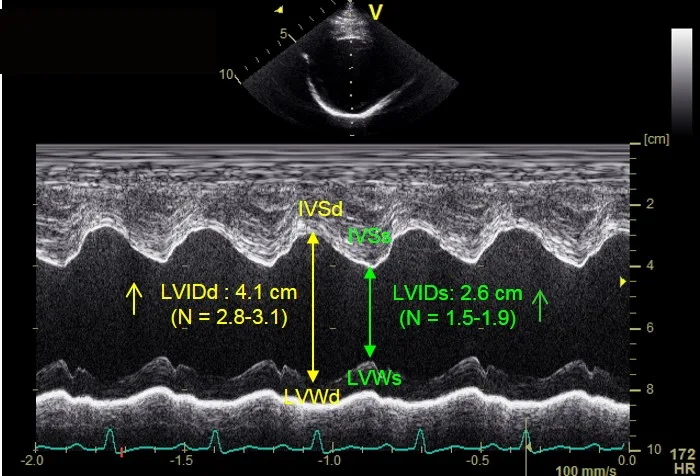
This Doberman pinscher was diagnosed with Stage B1 DCM, based on a ventricular premature contraction identified on an ECG and mild to moderate left ventricular systolic dysfunction. Figure 3A demonstrates left ventricular dimensions that are at the upper end of published normal for the breed during diastole (LVIDd) and an abnormal end systolic dimension during systole (LVIDs).
Stage B2 DCM
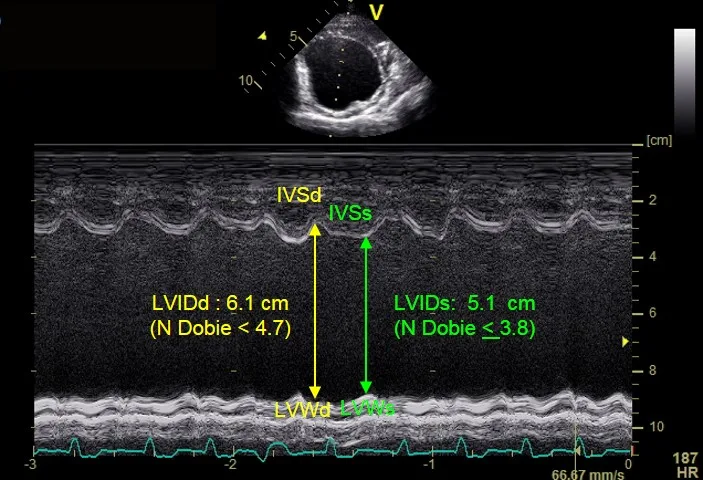
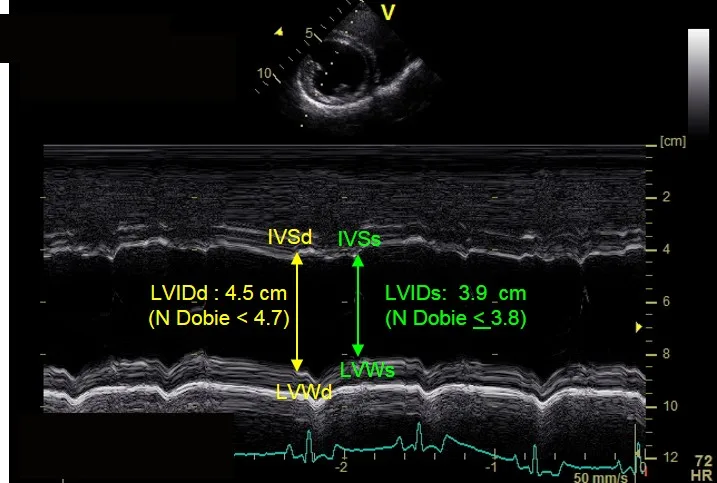
This Doberman Pinscher was diagnosed with Stage B2 DCM based on abnormal left ventricular measurements. Figure 4A shows left ventricular dimensions at the upper end of published normal for the breed during diastole (LVIDd) and an abnormal end systolic dimension during systole (LVIDs).
IVSd = interventricular septum in diastole, IVSs = interventricular septum in systole, LVIDd = left ventricular internal dimension in diastole, LVIDs = left ventricular internal dimension in systole, LVWd = left ventricular posterior wall in diastole, LVWd = left ventricular posterior wall in diastole, LVWs = left ventricular posterior wall in systole
The fractional shortening between these cases is similar (15% for Figure 3A and 11% for the Figure 4A); however, the LVIDd and LVIDs are extremely different as compared with normal values for the breed.
3. Echocardiographic Evaluation of Hypertrophic Cardiomyopathy
Diagnosis of hypertrophic cardiomyopathy (HCM) in a cat with a murmur is possible in general practice, but echocardiographic skills with basic imaging views must be perfected, as cats have small hearts with fast heart rates. Severe hypertrophy is relatively easy to identify, but more moderate and mild hypertrophy can be difficult to discern. Small or incorrect measurements can result in false positives, which lead to an incorrect prognosis given to owners.
Stage B1 HCM
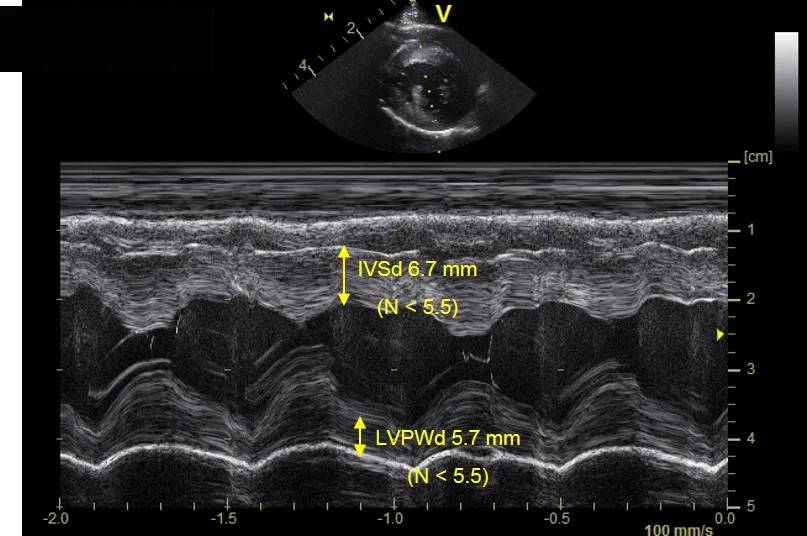
A clinically normal 7-year-old domestic shorthair cat with a loud murmur located at the left sternal border has only mild left ventricular hypertrophy and no left atrial enlargement based on echocardiographic evaluation. The patient has mild hypertrophy of the interventricular septum (IVSd 6.7 mm) and posterior wall during diastole (LVPWd 5.7 mm).
Stage B2 HCM
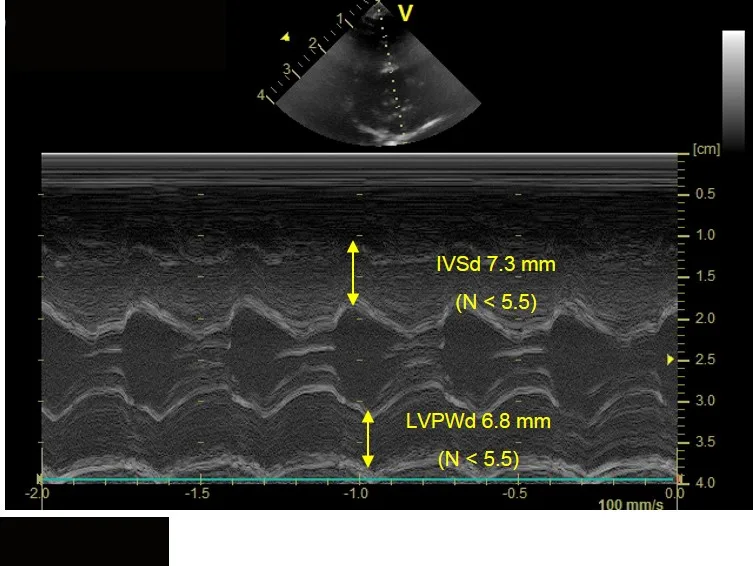
A clinically normal 3-year-old ragdoll cat with a loud murmur located at the left sternal border that demonstrates left ventricular hypertrophy (thickening) and left atrial dilation based on 2-dimensional echocardiographic evaluation. Figure 6A shows moderate-to-severe hypertrophy of the interventricular septum (IVSd 7.3 mm) and left ventricular posterior wall during diastole (LVPWd 6.8 mm).
IVSd = interventricular septum in diastole, LVPWd = left ventricular posterior wall in diastole
4. Echocardiographic Evaluation of Pleural & Pericardial Effusion
Evaluation for presence of fluid is a simple but important role of echocardiography in general practice. Suspected pericardial effusion can and should be evaluated promptly if suspected. If evidence of cardiac tamponade is present, therapeutic pericardiocentesis should be performed as soon as possible—without waiting for evaluation by a cardiologist. Many heart base and right atrial masses are visualized more easily when there is pericardial fluid surrounding the mass; thus, performing an echocardiographic evaluation before pericardiocentesis can offer valuable information regarding possible etiology and associated prognosis.
DCM = dilated cardiomyopathy, ECG = electrocardiogram, FS = fractional shortening, HCM = hypertrophic cardiomyopathy, LA:Ao = left atrial to aortic ratio, MMVD = myxomatous mitral valve disease, SAM = systolic anterior motion