Dysuria in a Cat: Could It Be More?
Chris Adolph, DVM, MS, DACVM (Parasitology), Zoetis Animal Health
Greg Nutt, DVM, Riverstone Animal Hospital, Canton, GA

History
Miss Kitty, a 9-month-old, intact, female domestic short-haired cat, presented with lethargy, vocalizing in the litter box, and bloody vaginal discharge of 3 days’ duration. The owners adopted Miss Kitty when she was 9 weeks of age. The kitten had not been vaccinated or dewormed, nor was she on any parasite preventive. Questioning revealed that, in addition to the presenting signs, Miss Kitty had been anorexic and vomiting for 3 days. She has been fed a dry over-the-counter cat food, and she had not been outside since adoption.
Physical Examination
The cat was bright, alert, and responsive on initial evaluation. Her temperature was 99.8°F (37.7°C), heart rate 180 beats/min, and respiratory rate 60 breaths/min, with a body condition score of 4/9. Mucous membranes were pale with a capillary refill time of 3 seconds. Flea comb examination revealed the presence of adult Ctenocephalides felis as well as flea frass. Cestode proglottids were present in the perineal region. A clear-to-pink vaginal discharge was noted. Abdominal palpation revealed cranial abdominal pain as well as a mildly enlarged and painful urinary bladder that was difficult to express.
Laboratory Diagnostics
Tests for FIV and FeLV were negative. CBC revealed a mild monocytosis and neutrophilia. A serum chemistry panel revealed azotemia and mild hyperglycemia (Table 1). Urinalysis via cystocentesis revealed concentrated urine with RBCs too numerous to count and mucus strands. The remainder of the urinalysis was within normal limits. No bacteria were seen. Urine culture was negative. Survey radiographs revealed a gas pattern in the GI tract, an enlarged bladder, and ileus throughout the small bowel (Figure 1). No stones were visible in the kidneys, ureters, bladder, or urethra.


Lateral (A) and ventrodorsal (B) radiographs showed a distended urinary bladder, ileus, and a GI obstructive pattern with possible gastric and small bowel foreign bodies.
Significant Laboratory Results
Too numerous to count
| NP | NP | 0-5 |
NP = not performed
Diagnosis
Jejunal tapeworm bezoar
Preliminary Diagnosis
Given the patient’s history and physical examination, the diagnostic differentials in this case included a functional urethral obstruction or bladder atony, lower urinary tract disease, GI foreign body, cestode infection, and flea infestation.
The owners declined additional diagnostics but did agree to an exploratory laparotomy based on concerns about GI foreign body and urinary tract disease.
Surgical Diagnostics
The patient was premedicated with dexmedetomidine (40 µg/kg), ketamine (5 mg/kg), and butorphanol (0.2 mg/kg), all given IM. She was induced with IV propofol to effect and maintained on inhalant 1% isoflurane for the duration of the procedure.
The urinary bladder was enlarged, discolored, and thickened. A catheter passed from the lumen of the bladder to the external urethra revealed no evidence of uroliths or mechanical obstruction. Tissue was obtained for histopathologic examination. The stomach was firm, and foreign material was suspected. Gastrostomy revealed a trichobezoar measuring 7.5 × 15.25 cm. Plication was noted in the mid-jejunal region. An enterotomy was performed, and a large mass of tapeworms—later identified as T taeniaeformis—was removed (Figure 2).
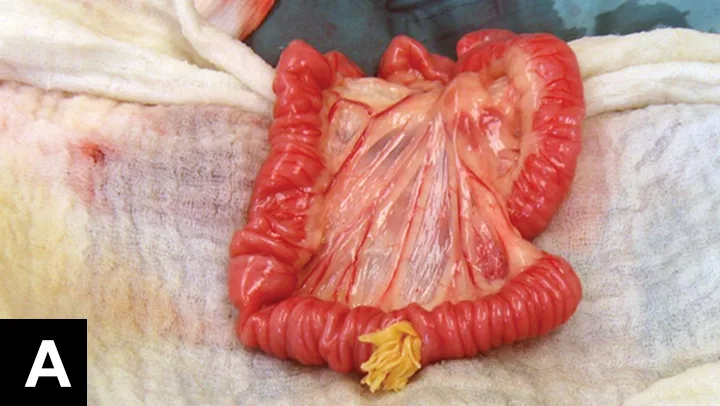

A large mass of T taeniaeformis was found and removed during an enterotomy.
Treatment & Outcome
After surgery, topical praziquantel–emodepside (12 mg/kg and 3 mg/kg, respectively) was administered, along with phenoxybenzamine (2.5 mg q24h PO). A recheck serum chemistry panel 3 days after surgery showed resolving azotemia. At 6 weeks postoperatively, Miss Kitty had complete resolution of both urinary and GI clinical signs. In addition, the azotemia had fully resolved.
Feline lower urinary tract disease is a common clinical disorder.1 The urinary bladder enlargement and dysuria in this case could be secondary to failure of bladder contraction, functional urethral obstruction, or a combination of both. Both neurogenic and nonneurogenic causes are possible, including spinal lesions, detrusor atony, detrusor-urethral dyssynergia, overdistension of the bladder, and idiopathic causes.5 The cause was not identified definitively in this patient.
Infection with T taeniaeformis is prevalent in cats.6,7 However, current detection methods overlook 87% to 90% of infections.8 It is likely that this patient acquired the tapeworm infection via predation prior to adoption. T taeniaeformis has been shown to live in a feline host for up to 34 months.2 Tapeworm-infected mice will come indoors, so the potential for predation and infection exists even in cats that never go outside.
Medical Treatment Options for Tapeworm Infection in Cats
Despite the low sensitivity of detection methods, fecal flotation and broad-spectrum deworming should be considered part of the workup and treatment for any cat that presents with GI signs. Surgical removal may be required for some tapeworm infections.9
Dipylidium caninum proglottids were not identified on the cat despite the presence of fleas. It is possible that these fleas did not harbor the metacestode for D caninum, or that flea infestation was recently acquired and within the 2- to 3-week prepatent period.