To Cut or Not to Cut: Poor Appetite in a Dog

Case & History
A 9-year-old castrated Yorkshire terrier has a three-day history of inappetence and one episode of vomiting. The patient was not eating his normal kibble but had eaten a small amount of chicken hand-fed by the owner.
Physical Examination
Abdominal palpation revealed cranial organomegaly, presumed to be hepatomegaly.
Laboratory Findings
The hematocrit value was normal; other relevant findings appear in the Table below.
Significant Laboratory Findings
ALT = alanine aminotransferase, ALP = alkaline phosphatase, GGT = γ-glutamyl transferase, WBC = white blood cell
Abdominal Radiographs
Left lateral (Figure 1A) and VD (Figure 1B) radiographs of the abdomen were obtained. Although thoracic radiographs were also taken, the findings were considered normal and, therefore, are not included here.


Left lateral (Figure 1A) and VD (Figure 1B) views of the abdomen.
Radiographic Findings
A mottled mineral opacity measuring ~12 mm in diameter is seen just caudal to the last right rib in the VD view, near the pyloroduodenal junction (Figure 2B, black arrows), and superimposed over the pylorus in the lateral view (Figure 2A, black arrows). This opacity could be a foreign body or a mineralized mass or lymph node. Heterogeneous soft tissue material, compatible with ingesta, is present in the gastric lumen as well as throughout the intestines, but no abnormal distention is evident. The liver extends past the costal arch with mild caudal displacement of the gastric axis, consistent with mild hepatomegaly; the margins are smooth. The remaining viscera and serosal detail are normal.
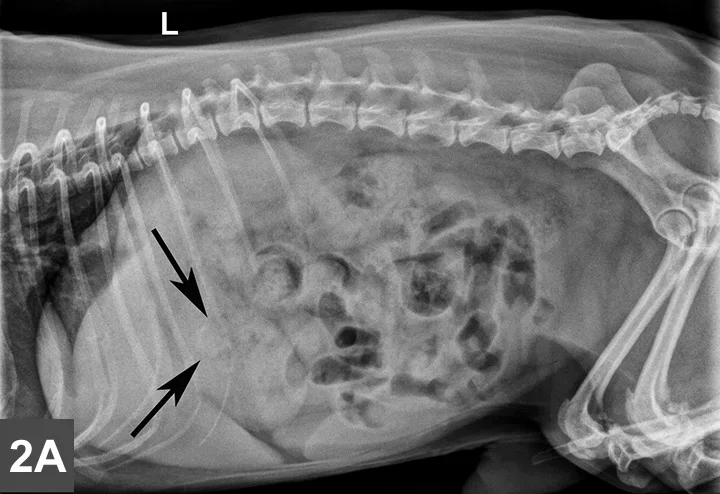
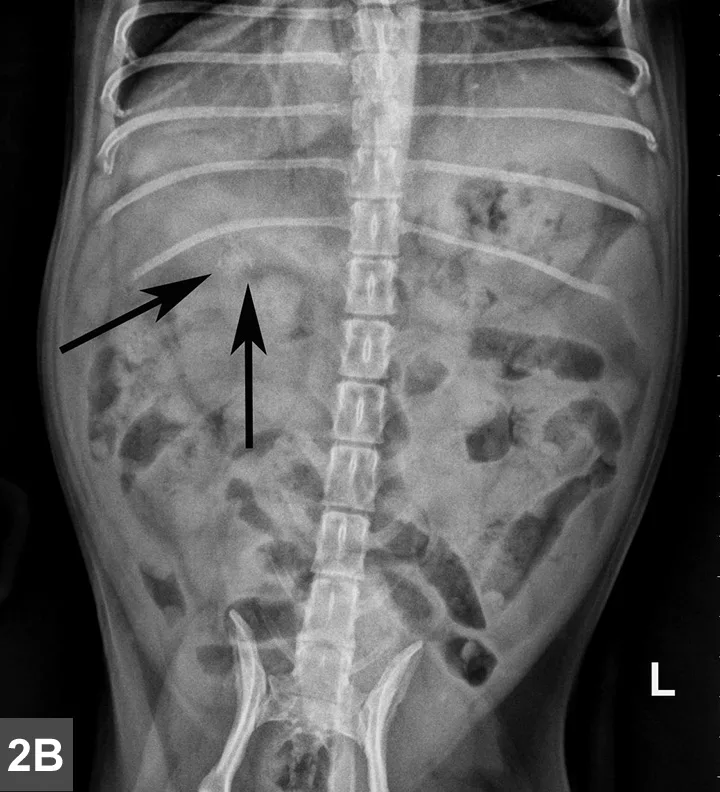
Same lateral and VD radiographs as in Figure 1A and B showing mineral density just caudal to the last right rib in the VD view (Figure 2B, black arrows) near the pyloroduodenal junction and in the lateral view (Figure 2A, black arrows) superimposed over the pylorus.
Should this patient go to surgery?
Presence of a foreign body could explain the small mineral density, inappetence, and vomiting; however, its location in the pyloric or duodenal lumen could not be confirmed in the VD view. In addition, presumed hepatomegaly on palpation and abnormal laboratory findings suggested hepatopathy with possible biliary obstruction. Considering the patient history and chemistry abnormalities, abdominal ultrasonography was recommended to identify the location of the mineralized structure and fully evaluate the GI tract and hepatobiliary system.
Abdominal Ultrasound Findings

The common biliary duct (CBD) is outlined by + markers while asterisks indicate the ribs.
On ultrasound imaging, the liver appears to be subjectively enlarged. The gallbladder appears severely distended with anechoic fluid; the cystic duct (0.60 cm in diameter) and common bile duct (CBD; 0.48 cm) adjacent to the right pancreatic lobe also appear distended (Figure 3A). Note that the ribs are causing beam attenuation. In addition, normal and abnormal diameters in dogs have not been reported; however, in one study in cats, extrahepatic biliary obstruction was involved when the ultrasonographic diameter of the CBD measured <5 mm.1
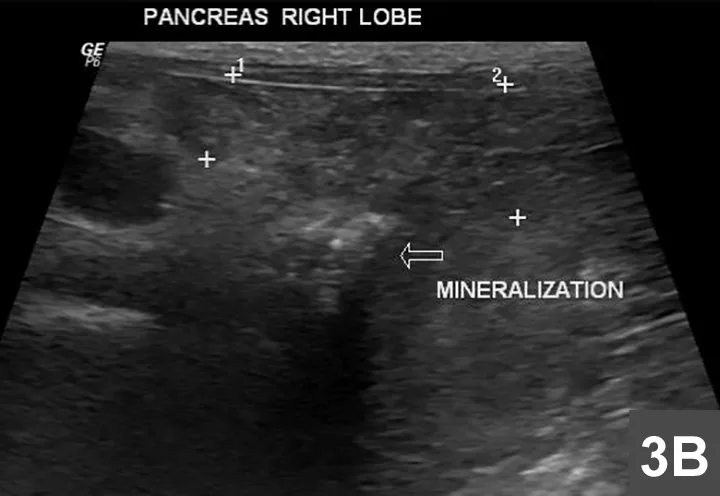
The + markers indicate a mildly heterogeneous pancreas, while the arrow indicates the region of mineralization associated with beam attenuation.
An area of beam attenuation compatible with mineralization also is visible in the region of the right pancreatic lobe, near the duodenal papilla (Figure 3B). The pancreas appears to be mildly heterogeneous and enlarged at this level, but the peripheral portion of the right pancreatic lobe is normal (homogeneous and much smaller).
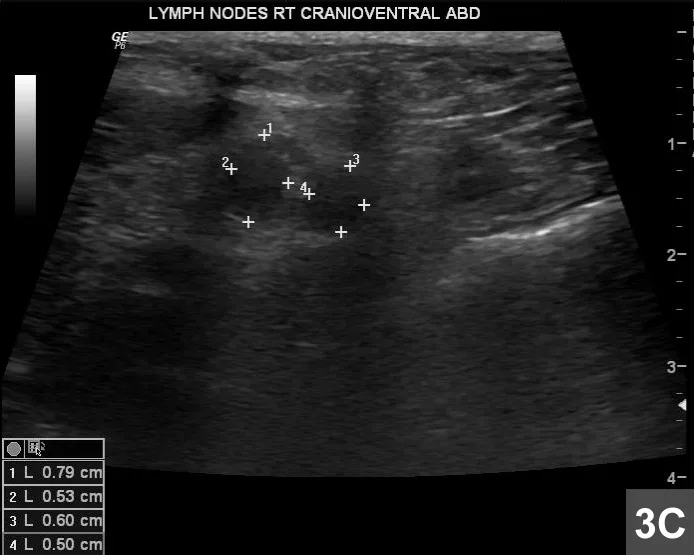
Paired hypoechoic lymph nodes in the right cranioventral abdomen (+ markers) are enlarged.
Pancreatic neoplasia was suspected based on a focal abnormal region with mineralization; its location in the right lobe was likely causing the CBD obstruction. Paired hypoechoic regional lymph nodes in the right cranioventral abdomen measuring 0.79 × 0.53 cm and 0.60 × 0.50 cm (Figure 3C) were suspected to be reactive or secondary to metastatic neoplasia. The remaining viscera were otherwise normal; no foreign body or other GI abnormality was detected, nor was free fluid.
Outcome
Pancreatitis was considered unlikely based on the focal abnormality with mineralization (pancreatitis tends to cause diffuse pancreatic enlargement and should not be mineralized) and the presence of regional lymphadenopathy. The abnormal region of the pancreas was aspirated under ultrasound guidance, and cytologic findings indicated neoplastic infiltration of the pancreas by a moderate to poorly differentiated carcinoma. One of the lymph nodes was also aspirated and showed metastatic carcinoma and marked suppurative necrotizing lymphadenitis. The patient had not been euthanized at the time of this write-up but was being treated with supportive care.
Comments
Extrahepatic bile duct obstruction in dogs is most commonly caused by extraluminal obstruction attributed to pancreatitis (19/45 cases; 42.2%) or neoplasia (11/45 cases; 24.4%).2 Pancreatic carcinomas in dogs are usually locally and extensively invasive and often metastatic at time of diagnosis; the prognosis is poor due to the critical location and advanced stage at diagnosis.3 The treatment options in metastatic pancreatic carcinoma are essentially palliative.