Chronic Vomiting & Diarrhea in a Dog
Michael E. Matz, DVM, DACVIM, Veterinary Specialty Center of Tucson, Arizona

Abigail, a 9.8-kg, 5-year-old spayed female beagle, presented with progressive vomiting and chronic diarrhea.
History
Vomiting and diarrhea were first noted 3 months earlier. The vomiting initially occurred once weekly but was now occurring almost daily. The vomitus usually contained bile-stained mucus. The diarrhea was characterized by normal frequency of bowel movements (2 times daily), decreased volume of stool per defecation, normal brown color, semiformed consistency, mucus, occasional occult blood, and tenesmus. No weight loss accompanied the vomiting or diarrhea and the dog's appetite remained normal.
There was one other dog in the household that was not showing clinical signs, and both dogs primarily stayed indoors. They ate a combination of dry and canned forms of a premium commercial diet and were on heartworm preventative (ivermectin plus pyrantel pamoate). No change of diet during the course of the illness was reported by the owners.
Recent diagnostics included abdominal radiographs (Figure 1) and trial therapy with metoclopramide (5 mg PO Q 8 H) for the vomiting and sulfasalazine (125 mg Q 8 H) for the diarrhea. Neither treatment resulted in any significant improvement.
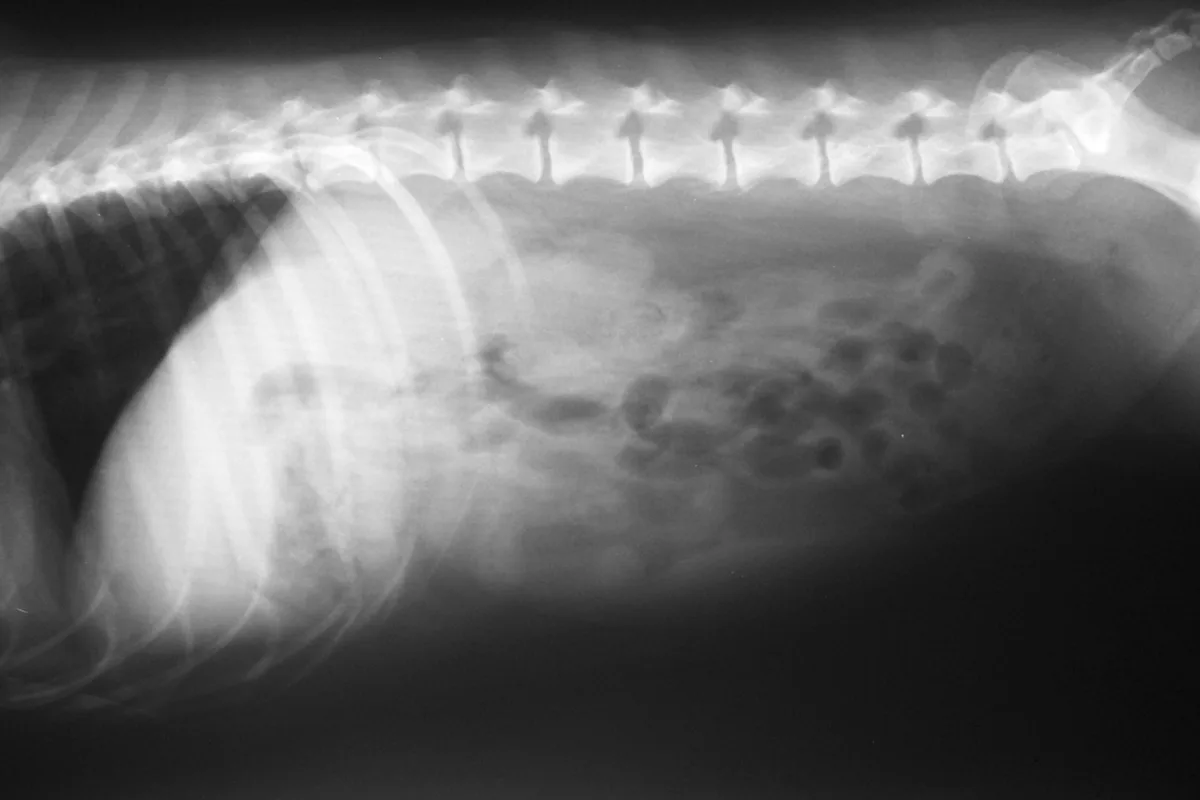
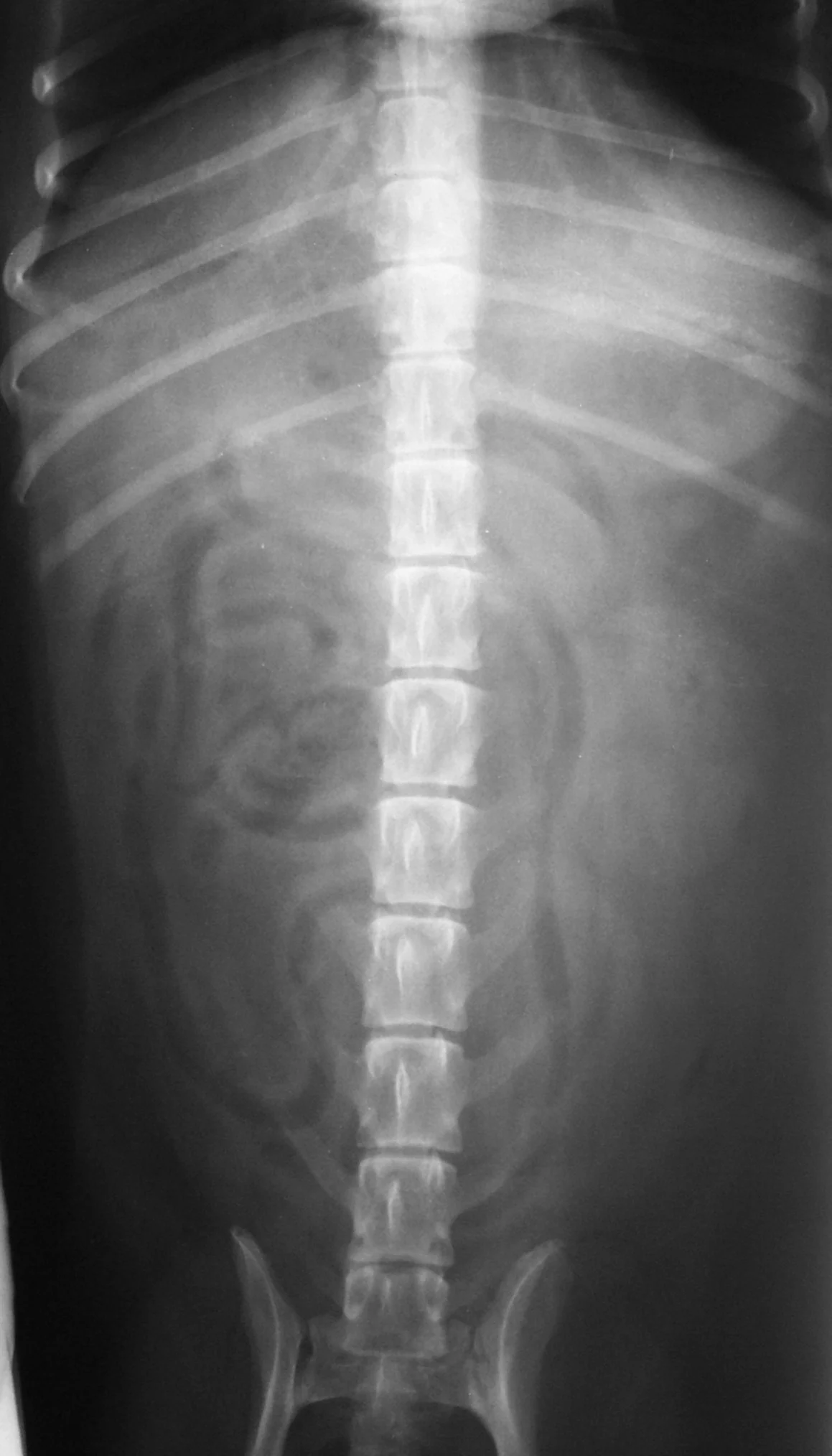
Lateral and ventral dorsal abdominal radiographs
Physical Examination
Upon presentation, Abigail was bright and alert. Her temperature, respiratory rate, and heart rate were within normal limits. Body condition was normal (5/9). Abdominal palpation and digital rectal examination were also normal. A small amount of brown pasty stool was obtained rectally.
Differential Diagnoses
Causes for chronic vomiting include primary gastrointestinal diseases and systemic diseases (Table 1). Causes for large bowel diarrhea include whipworms, diet (allergy, intolerance, response to fiber), inflammatory bowel disease (lymphocytic/plasmacytic, eosinophilic), irritable bowel syndrome, and colonic neoplasia.
Table 1: Common Causes of Chronic Vomiting in the Dog
Diagnostics
CBC, serum biochemical profile, and urinalysis (USG 1.027) were normal. Fecal flotation, using the zinc sulfate centrifugation technique, was negative for parasites. Abdominal ultrasonography was normal, although the stomach could not be completely assessed because of the presence of gas. These results were most consistent with primary gastrointestinal disease as the cause of chronic vomiting and diarrhea.
A dietary trial using a hypoallergenic (protein hydrolysate) diet containing a source of fermentable fiber (Hypoallergenic HP19, www.royalcanin.us) was begun. Fermentable fiber has a variety of beneficial effects on the large bowel, including increased mucosal surface-to-volume ratios, increased production of short-chain fatty acids, increased fecal bulk, and altered colonic transit rate.
Related Article: Managing the Vomiting Dog
Outcome
Diarrhea resolved within 10 days after the start of the dietary trial, but vomiting continued to progress. The trial was continued for 21 days. Abigail was now vomiting an average of twice daily. Upper and lower gastrointestinal endoscopy was recommended.
Ask Yourself...
What is your interpretation of the radiographs in Figure 1?
What is the purpose of a dietary trial?
Should endoscopic gastric and intestinal biopsies have been taken after discovery of the gastric foreign body and grossly normal duodenal and colonic mucosa?
Endoscopy
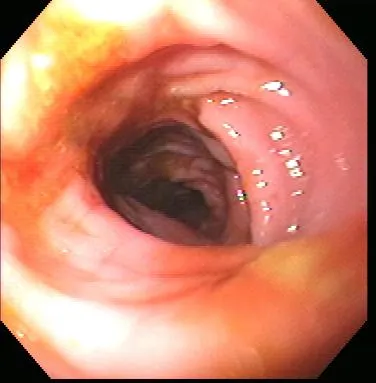
Gastroenteroscopy revealed a hard plastic foreign body (Figure 2) with curved, pointed ends. Points of the object were embedded in the gastric antral mucosa, resulting in hyperplasia. One of the curved points extended through the pylorus and hooked into the proximal duodenum (Figure 3). The endoscope could be passed around the foreign body into the duodenum, allowing biopsy of the duodenal mucosa. The gross appearance of the duodenal mucosa was normal (Figure 4). Attempts to remove the foreign body endoscopically were unsuccessful. Before the dog was sent to surgery for removal of the foreign body, colonoscopy was performed. The colon appeared normal on gross inspection (Figure 5). Biopsies were obtained from the cecum; ascending colon; transverse colon; and proximal, middle, and distal descending colon. At surgery, a gastrotomy incision was made in the pyloric antrum and the foreign body was forcefully removed. It was a plastic object used to secure the legs of a turkey carcass.
Histologic evaluation of the endoscopic biopsy samples of both the duodenum and colon demonstrated a mild to moderate infiltrate of increased numbers of eosinophils intermingled with a background population of lymphocytes and plasma cells within the lamina propria.
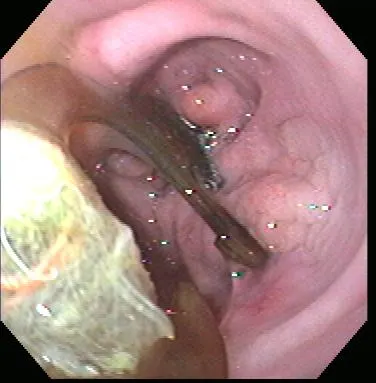
Endoscopy of the gastric antrum showing the foreign body and the mucosal proliferation induced by its presence

Endoscopy of one end of the foreign body hooked around the pylorus

Healthy proximal duodenum
Healthy descending colon
Diagnosis: Gastric foreign body and diet-responsive diarrhea vs inflammatory bowel disease
Although epithelial changes are described in many histologic classification schemes proposed for inflammatory bowel disease-often for more severe histologic grades-there are schemes where the histologic findings of this case would be classified as inflammatory bowel disease. The World Small Animal Veterinary Association is presently attempting to establish uniform clinical and histologic criteria for the diagnosis of inflammatory bowel disease; however, their recommendations have yet to be published.
The characteristics of the diarrhea in this case are most consistent with large bowel diarrhea (Table 2). The presence and increasing frequency of vomiting could indicate concurrent gastritis or a diffuse gastrointestinal disease process (gastroenterocolitis), although vomiting can be observed in patients with large bowel diarrhea.
Treatment
Abigail was continued on the hypoallergenic diet alone after removal of the gastric foreign body.
Table 2: Localization of Chronic Diarrhea
Outcome
No vomiting or diarrhea had been observed 10 weeks after surgical removal of the foreign objects. Resolution of the large bowel diarrhea with dietary therapy supported a diagnosis of an adverse reaction to food. Based on history, it is possible that the vomiting initially resulted from an adverse reaction to food, with frequency worsening only after ingestion of the gastric foreign body. A true food sensitivity could be ruled out only by showing recrudescence of clinical signs on reexposure to the offending diet or by feeding an elimination diet and reintroducing possible allergens one at a time.
Did You Answer...
Abdominal serosal detail is adequate. There is no evidence of radiopaque gastrointestinal foreign bodies or intestinal obstruction. The remaining abdominal and extraabdominal structures are within normal limits.
Some adverse reactions to food are mediated by the immune system-that is, food allergies-and some are not, such as food intolerances. These adverse reactions may produce an inflammatory response that is indistinguishable from inflammation from other causes (ie, inflammatory bowel disease). To help eliminate adverse reactions to food as a cause of chronic vomiting and/or diarrhea, a dietary trial using a protein hydrolysate diet, or less preferably, a novel protein source diet, should be performed.
Protein hydrolysate diets are based on protein sources that have been enzymatically cleaved into small peptides. The peptide fragments are less likely to stimulate mucosal mast cell degranulation or escape the digestive process and gain access to the immune system. For this reason, protein hydrolysate diets are more likely to achieve long-term clinical response compared with novel protein diets. The diet should also include highly digestible carbohydrates and fats, be gluten- and lactose-free, and restrict use of additives and preservatives to reduce the likelihood of food intolerances.
A dietary trial should be conducted for 2 to 4 weeks to assess its efficacy. However, a response is often seen more rapidly (days) in dogs with adverse reactions to food, as was oserved in this case.
In this case, the foreign body could have contributed to the vomiting but may not have been the sole cause (it could have accounted for the apparent progressive course). Gastrointestinal biopsy specimens should always be obtained during endoscopy to investigate the cause of chronic vomiting and/or diarrhea, even if the gastric and intestinal mucosa appear normal.