Chronic Otitis Externa
Susan Paterson, VetMB, MA, DVD, DECVD, FRCVS, Virtual Vet Derms, Kendal, United Kingdom

Rolo, a 4-year-old Labrador retriever, was presented for recurrent bilateral otitis externa.
History
The owner reported a 2-year history of recurrent otitis externa. A review of medical records revealed that Malassezia pachydermatis was repeatedly cultured from the ears. Each episode of otitis responded to topical otic preparations, but there was a consistent pattern of relapse shortly after discontinuation of therapy. Rolo did not respond to an 8-week food trial (home-cooked fish and potato diet). There was no seasonal pattern to the otitis. He actively participated in bird hunting and swam regularly.
Physical & Dermatologic Examination
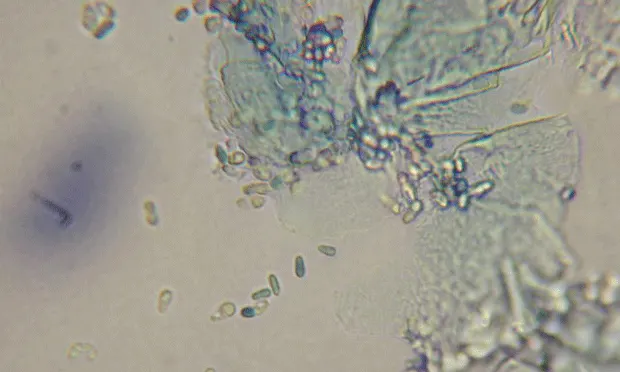
Erythema of the ear pinnae was present in addition to ceruminous discharge in both ear canals. The rest of the physical examination was unremarkable. The dog was sedated to examine his ears more thoroughly. Routine otoscopy revealed erythema and hyperplasia of the canals; both ear drums were intact and appeared normal (Figure 1). After otoscopic assessment and before cleaning was performed, ear wax from both ears, stained with Rapi Diff, was examined and revealed large numbers of Malassezia pachydermatis (Figure 2 above: “Peanut”-shaped yeasts typical of Malassezia pachydermatis).
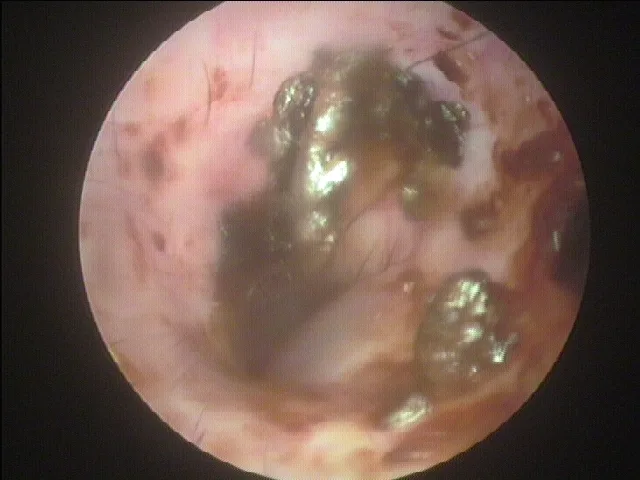
Videootoscopy image of the ear canal showing hyperplasia and erythema
Ask Yourself
Why has this problem recurred?
How should the case be investigated?
Is it important to know that the dog swims?
Diagnosis:
Atopic otitis externa with secondary Malassezia overgrowth
Ear disease will recur if the inciting trigger is not identified and treated. Examples of primary triggers for otitis in the dog are listed in the Table.
Perpetuating factors
Infection/overgrowth with Malassezia species is a perpetuating factor. Perpetuating factors complicate ear disease but do not initiate it. Malassezia overgrowth often perpetuates allergies or hypothyroidism. Other perpetuating factors for ear disease include bacterial infection, chronic changes in the ear canal (stenosis, ceruminous gland hyperplasia), and otitis media.
Table: Otitis Externa in the Dog—Triggers
Diagnostics
Investigation of recurrent ear problems focuses on identifying underlying skin disease and treating any perpetuating factors. Pinnal and ear canal examination can give some indication of primary disease (Table). Routine cytology and mineral oil preparations to examine ear exudates for parasites are necessary. Culture of ear canal exudate is indicated when rods, white blood cells, and/or mixed bacterial flora are seen.
Because the most common underlying triggers for recurrent otitis externa are allergies and endocrine disease, identification of the cause may require, but not be limited to, routine hematology, serum biochemical profiles, endocrine panels, food trials, and in vitro or in vivo allergy testing. In some cases, biopsy of the skin/ear tissue and computed tomography or magnetic resonance imaging may be needed, especially if otitis media is suspected as a perpetuating cause of otitis externa.
Allergy testing & cytology
Since a proper food trial had been performed in this patient prior to examination, intradermal allergy testing was pursued. Strong positive reactions to Dermatophagoides pternoyssinus and Dermatophagoides farinae were noted. This result suggested that environmental allergy/atopy was the primary trigger for the recurrent yeast otitis.
Routine and video otoscopic examination of the vertical and horizontal ear canal revealed hyperplasia but no evidence of chronic changes; the tympanic membranes were normal, which indicated that otitis media was unlikely. Malassezia pachydermatis was the only organism identified on cytology, strongly suggesting that Malassezia was the sole perpetuating factor.
Did You Answer...
The otitis is recurring because the underlying trigger has not be identified and treated. Although ectoparasites, such as Otodectes and Demodex, can cause disease in young dogs, when Malassezia is found as a secondary infection in a young dog with recurrent bilateral otitis, allergy is the most likely trigger.
Investigation involves examination of the pinnae, ear canal, and tympanic membrane; cytology of ear exudates; and diagnosis of possible underlying allergies through food trials and in vitro or in vivo intradermal allergy testing.
Swimming is a predisposing factor in otitis externa, especially in allergic dogs. An ear cleaner that has activity against yeast, such as one containing boric acid, should be included in management. In addition, owners can be educated about ear care and taught to look for early signs of ear disease.
Predisposing factors
Allergies alone can predispose dogs to Malassezia overgrowth; however, activities such as swimming further complicate disease. Chronic wetting of the inside of the ears causes maceration of the skin and predisposes dogs to Malassezia overgrowth.
Predisposing factors do not lead to ear disease but can make its development more likely and management of primary ear disease difficult. Other predisposing factors include conformational changes such as hairs in the ear canal or ear canal stenosis, or pendulous pinnae. In this dog the only predisposing factor present was wetting of the ear due to swimming.
Management
Management includes otic preparations containing steroids and antimicrobials that have a spectrum of activity against yeast. In this patient, long-term therapy involved allergy-specific immunotherapy and regular cleaning of the ears with a boric-acid–based cleaner after swimming. In some cases, especially if the dog’s ears are painful, systemic antifungals, such as ketoconazole or itraconazole, are needed.