Cataracts in Dogs
Laura Mancuso, VMD, University of Tennessee
Diane Van Horn Hendrix, DVM, DACVO, University of Tennessee, Knoxville
How do I approach a suspected cataract in a canine patient?
Overview1
Cataracts may occur at any age and in any location in the lens. Location may predict progression risk. Cataracts partially or completely block tapetal reflection and fundic examination and are often classified by stage of maturation and cause.
Stages of Maturation
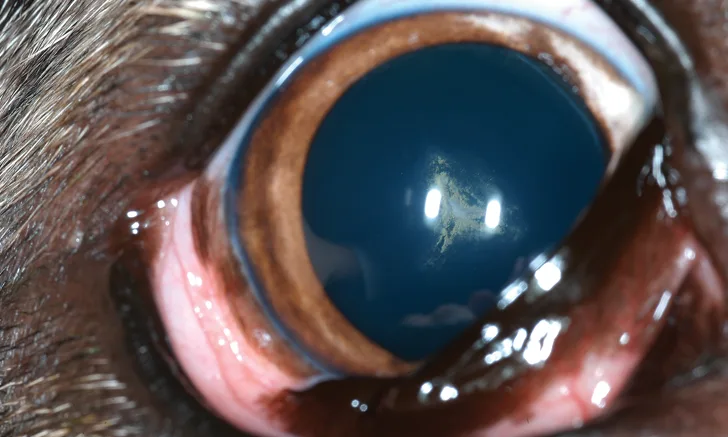
Incipient (Figure 1): <15% lens volume. Tapetal reflection is minimally obstructed. Visual deficits are not apparent.
Immature (Figure 2): 15% to 99% lens volume. Tapetal reflection is still visible but varies with the degree of cataractous lens. Visual impairment is variable, from minimal to near-complete blindness. Note that partial tapetal reflection and vision may be restored during cortical resorption in hypermature cataracts. This can confound the distinction between hypermature and immature cataracts.
Mature (Figure 3): 100% lens volume with no resorption. No tapetal reflection is visible. Eyes are blind but retain dazzle reflex and pupillary light reflexes (PLRs) if the retina is functional.
Hypermature (Figure 4): Resorption is present and produces a wrinkled anterior lens capsule with white plaques and multifocal sparkling. Phacolytic uveitis is common.
Morgagnian: Resorption and liquefaction of lens cortex with ventrally positioned (ie, dependent) nucleus. Vision may return.

FIGURE 1
Incipient cataract
Causes
Primary Cataracts2
Primary cataracts have a genetic basis and occur without exogenous insult or metabolic disease. They frequently occur bilaterally and are typically symmetrical. Clinicians should consult the literature for specific appearance in at-risk breeds and inform breeders of suspected primary cataracts to prevent perpetuating the heritable condition.
Heritable cataracts are the most common presentation in dogs and may occur in juvenile or adult dogs of many breeds. Bilaterally symmetrical cataracts with a hallmark, breed-related appearance and/or location in a young-to-middle-aged purebred dog are diagnostic. Progression varies among breeds and individual patients. Few breeds have proven mechanisms of inheritance or genetic tests available. Consulting the literature is recommended, as is examination of the patients parents and littermates when possible.
Some congenital cataracts are primary and inherited, as exemplified in some breeds (eg, miniature schnauzer, Boston terrier). Parents and littermates should be examined when possible.
Secondary Cataracts
These cataracts occur secondary to exogenous insult or concurrent disease processes (ocular or systemic). Categories include diabetic, uveitic, hypocalcemic, degenerative, traumatic, nutritional, radiation-induced, and toxic.
Diabetic
Diabetic cataracts are the second most common cataracts in dogs. With hyperglycemia, sorbitol accumulates in the lens and causes osmotic draw and disruption of lens fibers. Diabetic cataracts begin as vacuoles at the equator and are most easily visible following pharmacologic dilation, then progress quickly and become swollen. They can produce visible Y sutures and phacolytic uveitis and create risk for lens capsule rupture. In a historical or undiagnosed diabetic patient, acute-onset blindness with eyes concurrently clouding over is a classic presenting complaint. Most diabetic dogs (75%) develop cataracts within 6 to 12 months of disease onset, even when regulated.3 Dogs with acute cataract development should be screened for diabetes mellitus.
Uveitic
Intraocular inflammation of any cause can result in cataract development. All cataracts, regardless of cause, may cause phacolytic uveitis. This can make it difficult to determine whether a cataract is the cause or result of uveitis. If uveitis preceded cataractogenesis, systemic diagnostics are warranted. It is important to rule out neoplastic, infectious, and inflammatory diseases.
Hypocalcemic
Hypocalcemic cataracts commonly occur secondary to metabolic disease (eg, primary hypoparathyroidism) rather than nutritional deficiency. These cataracts present as classic multifocal white pinpoints or as a field of stars within the lens cortices. In 1 study, cataractogenesis occurred in 32% of hypocalcemic dogs with primary hypoparathyroidism.4 Care should be taken not to mistake asteroid hyalosis in the vitreous for hypocalcemic cataracts, as both are multifocal and star-like.
Degenerative
As in humans, age-related cataracts develop in dogs. Appearance and progression of degenerative cataracts is variable, and diagnosis is based on exclusion and signalment. Differentiation between genetic and degenerative cataracts is rarely possible. For large breeds, degenerative cataracts should be suspected in patients 6 years of age; for small breeds, degenerative cataracts should be suspected in patients >10 years of age.1
Traumatic
Cataracts can result from penetrating trauma from a sharp object (eg, cat claw, plant thorn). Severe uveitis secondary to blunt trauma, corneal trauma, or foreign material in the anterior chamber can also cause cataract development. A small rent in the lens capsule can cause a focal cataract and then self-seal with no or minimal progression. However, in some animals, severe uveitis may occur after a period of quiescence. This indicates septic implantation syndrome, which occurs when bacteria are implanted in the lens during the initial injury. A large lens capsule tear may occur with sharp penetrating trauma, most commonly a cat claw. This often results in severe, intractable (ie, phacoclastic) uveitis and often necessitates enucleation. Cataracts can also result from electrocution secondary to a lightning strike or chewing wires.
Nutritional5,6
When fed exclusively, inappropriate milk replacers that are amino acid-deficient may cause cataracts in puppies. Because of their neonatal onset, nutritional cataracts are most often isolated to the nucleus, at least initially. Thorough history and littermate examination is essential. Supplementation with dams milk or appropriate puppy milk replacer can prevent cataract formation and progression. Once the puppy is on a balanced puppy food diet, nuclear cataracts will often condense as new lens fibers are laid down.
Radiation-Induced
If eyes are in the exposure field during radiation therapy, cataracts may form 6 to 12 months after insult.7 A thorough history is essential. Other signs (eg, conjunctivitis, keratoconjunctivitis sicca [KCS], keratitis, retinopathy) may also occur secondary to radiation.
Toxic
During retinal degeneration, progressive retinal atrophy (PRA), and retinal detachment, dying photoreceptor cells are hypothesized to produce toxic aldehyde metabolites that progressively damage the lens.8 However, in at-risk breeds, concurrent cataracts and PRA may represent 2 separately inherited diseases occurring together. Certain medications (eg, ketoconazole administered at high doses,9 dimethyl sulfoxide used long-term10) may cause lenticular damage. Identifying retinal degeneration is difficult when fundic examination is impaired. Thus, pre-operative screening with an electroretinogram is essential before cataract surgery, as phacoemulsification will not restore vision without a functional retina.
Location1
Cataract location within the lens may provide clues about cause and risk for progression. Accurately describing a cataracts location in medical records also helps track progression over time.
Subcapsular: Within the cortex, adjacent to the anterior or posterior lens capsule. These cataracts are frequently heritable and variably progressive.
Cortical: Within the anterior or posterior cortex, potentially both. Progressive cataracts in any location eventually expand into the cortex.
Equatorial: At the lens periphery, closest to the lens zonules. Typically progressive, as lens growth is active at the equator. Diabetic cataracts begin as equatorial vacuoles.
Nuclear: Within the lens nucleus. Almost always congenital or neonatal (primary or secondary). Nuclear cataracts rarely progress.
CBC = complete blood count, IOP = intraocular pressure, KCS = keratoconjunctivitis sicca, NSAID = nonsteroidal anti-inflammatory drug, PLR = pupillary light reflex, PRA = progressive retinal atrophy
Examination
A complete ophthalmic examination should be performed and should include examination of PLR and menace response, Schirmer tear test, fluorescein stain, intraocular pressure (IOP), aqueous flare and lens assessment, and a fundic examination if possible. A complete physical examination is also pertinent, as cataracts may be related to extra-ocular disease.
Pupillary Light Reflexes & Menace Response
Assessments of dazzle reflexes and PLRs test subcortical, unconscious reactions to light; they do not test vision. If the patient has a functional retina, these reflexes should be present with all cataract stages. Menace response is a rudimentary test for vision. In patients with cataracts, menace response may be present, equivocal, or absent, depending on the stage of maturation.
Schirmer Tear Test
Less than 15 mm of wetting in 60 seconds indicates inadequate aqueous tear production.
Fluorescein Stain
Positive fluorescein stain indicates a break in corneal epithelium (ie, corneal ulcer).
Intraocular Pressure
IOP >25 mm Hg is abnormal and indicates underlying glaucoma.
IOP <15 mm Hg may be abnormal and indicate underlying uveitis. In a cataract patient, phacolytic (ie, lens-induced) uveitis should be suspected and treated with topical ophthalmic anti-inflammatory drugs (steroidal and/or nonsteroidal) 1 to 4 times a day, depending on severity.
Anterior Chamber Examination
Using a slit-beam (available on most direct ophthalmoscopes) aids in visualization of free-floating cellular or proteinaceous debris within the aqueous humor (ie, aqueous flare). Such debris indicates intraocular inflammation.
Lenticular Examination
Retroillumination with a transilluminator or penlight can help identify tapetal reflection obstruction. Direct illumination can help localize the opacity within the lens.
Fundic Examination
If IOP is normal or low, a short-acting topical mydriatic (eg, tropicamide) should be instilled; after pupillary dilation (15-20 minutes later), direct or indirect ophthalmoscopy should be performed to assess for retinal or optic nerve pathology that may contribute to visual deficits.
Opacity
The lens opacities may not be of the severity to explain severe visual deficits (consider retinal, optic tract, or visual cortical lesions). In addition, cataracts alone will never alter the PLR. When the PLR is absent or decreased, iris atrophy, retinal, optic tract, or oculomotor nerve lesions should be considered. Evidence of PRA or retinal detachment may be visible on ophthalmoscopy. If the fundus is not visible or findings are equivocal, electroretinography and ocular ultrasonography are required to confirm retinal status.
Extralenticular Opacities
Pet owners often incorrectly describe corneal and anterior chamber opacities as cataracts. Common pretenders include but are not limited to corneal lipid or calcific degeneration, corneal endothelial degeneration or dystrophy, corneal edema, and lipoid aqueous humor.

Nuclear sclerosis
Nuclear Sclerosis
Nuclear sclerosis, an aging change in dogs age 7 years or older, results from increased density of the lens nucleus. It is most often represented by a spherical haze in the axial lens (Figure 5), which does not block tapetal reflection. Pharmacologic pupillary dilation helps identify nuclear sclerosis, as a dense nucleus mimics an immature or nuclear cataract when the pupil is miotic. When the pupil is dilated, the surrounding cortex should be clear and the fundus visible. Older dogs may have both nuclear sclerosis and cataracts, but no treatment or monitoring is indicated for nuclear sclerosis alone.
Treatment
Once a cataract forms, surgery is the only treatment method to restore vision. Phacoemulsification uses ultrasonic energy to fragment and extract cataractous lens material from its capsular bag. An artificial intraocular lens is placed in the empty capsule with routine cataract surgery. Electroretinography and ocular ultrasonography are standard pre-operative screening tools to confirm an eyes candidacy for cataract surgery. Although pre-operative preparation and postoperative management can be intensive, canine cataract surgery is often successful and rewarding (Figure 6). Risks, time commitment, and financial demands of phacoemulsification should be discussed with the pet owner.

Re-examination of a postoperative patient 15 months postphacoemulsification. The artificial lens can be seen within the lens capsule.
See Management Tree: Cataracts in Dogs for an algorithmic approach to evaluating and treating cataracts in canine patients.
Pre-operative Screening
Pre-operative screening should be performed because lens opacity obstructs posterior segment examination. Electroretinography confirms the retina is electrically functional and rules out advanced retinal degeneration. Ocular ultrasonography confirms the posterior segment is structurally sound; this rules out retinal detachment and posterior lens capsular rupture. If an eye fails either test, phacoemulsification is unlikely to improve vision and is not indicated.
Concurrent Ocular or Systemic Disease
Phacolytic Uveitis1
Intraocular inflammation secondary to leakage of antigenic lens protein is the most common complication of untreated cataracts and can cause corneal endothelial damage, synechiae, and secondary glaucoma long-term. Risk for secondary glaucoma and postoperative complications increases with time. If phacoemulsification is being considered, aggressive treatment with ophthalmic steroids and topical ophthalmic NSAIDs (eg, flurbiprofen, diclofenac, ketorolac) and a mydriatic are indicated. Generally, uveitis must be controlled before surgery. Because long-term topical ophthalmic steroids negatively impact corneal health, uveitis should ideally be controlled with topical ophthalmic NSAIDs (ie, flurbiprofen, diclofenac, ketorolac) when surgery is not being considered.
Diabetes Mellitus
Diabetes must be well-controlled before cataract surgery because of general anesthetic concerns and anticipated glycemic disruption from general anesthesia, recovery, and topical ophthalmic steroids. A fructosamine test and urine culture are often performed as part of the diabetic work-up. Diabetic cataracts tend to progress quickly, and risk for secondary glaucoma and postoperative complications increases with time. When possible, topical ophthalmic NSAIDs should be used to control anterior uveitis.
Surgical Notes
The older the cataract is, the harder the lens material becomes. This may increase complications following phacoemulsification (ie, surgical removal of cataracts) because of longer duration of surgery and greater ultrasonic energy required.
Alternative procedures (ie, intracapsular lens extraction, sulcus intraocular lens placement) are used only when complications (ie, capsular tear or rupture, lens subluxation) arise, are anticipated, or are already present.
A complete ophthalmic examination (ie, Schirmer tear test, fluorescein stain, IOP), physical examination, blood work (ie, CBC, serum chemistry profile), and urinalysis should be performed for all cataract patients pre-operatively.
For at-risk breeds, pre-operative retinopexy may be recommended to reduce the likelihood of retinal detachment.13
If the dog is fractious for administration of eyedrops or owner compliance is variable, the patient may not be a surgical candidate.
Electroretinography and ocular ultrasonography are normal in patients with blindness originating behind the retina, as in optic tract or visual cortical lesions.
Glaucoma
Elective phacoemulsification on historically glaucomatous eyes, even those controlled medically, is extremely risky.11 Cataract surgery with concurrent laser ablation of the ciliary body can be attempted in select cases.
Lens Subluxation or Luxation
Lens subluxation may not preclude cataract surgery, but it increases complication risk and may necessitate conversion to intracapsular lens extraction (ie, intracapsular cataract extraction). Uveitic damage to lens zonules leads to increased risk for subluxation or luxation of cataractous lenses.
Corneal Disease
Impaired healing of corneal incisions can have catastrophic consequences. Corneal disease (eg, KCS, corneal ulcers) must be well-controlled or resolved before phacoemulsification. Additionally, corneal opacities can obscure visualization of the lens during surgery, thereby precluding surgery.
Retinal Degeneration or Detachment
Patients are not surgical candidates if blinding retinal lesions are confirmed or suspected in the affected eye(s).
Other Systemic Disease
Especially pertinent are concurrent conditions that make the patient a poor general anesthetic candidate (ie, cardiovascular, respiratory, or renal compromise).
Postoperative Complications
Prognosis for vision after phacoemulsification is between 80% to 95%, but blinding complications exist and certain breeds are at higher risk.12
Retinal detachment is the most common postoperative complication (8.4%) and can be immediate or delayed; it is blinding but nonpainful, so enucleation is not warranted.12 Bichons frises, shih tzus, and Boston terriers are at increased risk. A few veterinary specialty centers in the United States offer retinal reattachment surgery.
Glaucoma is the second most common postoperative complication (6.7%).12 Boston terriers and Labrador retrievers are at increased risk.14 Postoperative ocular hypertension may be transient or persist. Antiglaucoma topical ophthalmic medication (eg, dorzolamide, timolol, latanoprost) may be required on a case-by-case basis, depending on postoperative ocular hypertension severity. Post-operative IOP rechecks are essential. Even if previously normal, postphaco- emulsification eyes are considered to be at a lifelong increased risk for glaucoma. If medically refractory, secondary glaucoma can be blinding and painful, thus necessitating enucleation.
Postoperative Management
Postoperative management is intensive and demanding but integral to success. Pet owners should be prepared for rigorous postoperative eyedrop regimens. It is common for 4 to 5 topical opthalmic solutions to be applied 4 to 6 times a day for several weeks. Pet owners should also be prepared for frequent postoperative rechecks. Scheduling recommendations vary significantly, depending on individual complications. To protect the integrity of corneal sutures, an Elizabethan collar is typically recommended for 2 to 3 weeks postoperatively.
Management Tree

