Canine Oral Pathology

In the clinical setting veterinarians often rely on oral examination to determine if a dental procedure is required. However, subgingival pathology may go undiagnosed. Two important veterinary dentistry diagnostic tools are the dental probe/explorer and dental radiography. The dental probe/explorer helps determine periodontal pocket depth and evaluate exposed pulp chambers and enamel defects; dental radiography assists in the discovery of subgingival pathology not visible during oral examination.
While periodontal disease is the most common oral disease, other pathologic conditions occur and are more difficult to diagnose without dental radiography or histopathology. This article demonstrates the benefit of dental radiography in identifying oral pathologic conditions.
The following photographs illustrate a variety of oral pathologies in the dog. Choose from the diagnoses listed; each disease corresponds with only 1 choice. This list of diagnoses is not exclusive. Many other dental pathologic conditions exist.
1. Acanthomatous ameloblastoma (acanthomatous epulis)
Intraoral radiography of the gingival mass demonstrated bony involvement (arrowhead). Histopathologic evaluation diagnosed the mass as an acanthomatous ameloblastoma, which is classified as a benign odontogenic tumor. The metastatic potential for this tumor is not known; however, it is locally aggressive, infiltrating surrounding tissues. Treatment options include surgical excision with 1-cm margins (the treatment of choice) or radiation therapy. Recurrence after incomplete excision is common. The uncomplicated crown fracture of #304 (arrows) was an incidental finding.
2. Periapical bone lysis
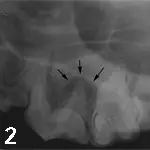
This intraoral dental radiograph of the left maxillary fourth premolar tooth (#208) demonstrates loss of bone structure around the root tip (periapical region) resulting in a radiolucent area (arrows). Periapical lysis is a radiographic sign of endodontic disease that is commonly associated with irreversible pulpitis or necrotic pulp. If left untreated the disease process continues with destruction of the surrounding bone. Endodontic therapy is required for the tooth to be maintained; otherwise extraction is indicated.
3. Immature nonvital tooth

A complicated tooth fracture of the left mandibular canine tooth (#304) resulted in an immature nonvital tooth. This is demonstrated by the widened pulp cavity. As teeth mature, odontoblastic cells that line the pulp form secondary dentin, decreasing the diameter of the canal. The width of the canal and the open apex indicate that this fracture occurred when the patient was less than 1 year of age. Nonvital teeth require endodontic therapy or extraction.
4. Gemination

The gross image and intraoral radiograph show 2 crowns on the right maxillary second incisor tooth (#102). Observe the 2 pulp chambers merging into a single root canal in the radiograph (arrow). Single incisor tooth gemination is common in dogs and occurs when a single tooth attempts to form 2 teeth, resulting in partial division with a common pulp chamber. The result is crowding between the 2 crowns; therefore, treatment is aimed at preventing periodontal disease. Note the presence of gingivitis around #102.
5. Tooth luxation

In the gross image the left mandibular canine tooth (#304) is laterally luxated (arrows ) with a fracture of the buccal alveolar bone plate. The intraoral radiograph demonstrates displacement of #304 within the alveolus; observe the space between the root apex (arrow) and the bottom of the alveolus (arrowhead ). Luxation injury is defined as the displacement of the tooth within the alveolus. Treatment for luxation injuries involves reimplantation and stabilization of the tooth within a few hours of the injury. Endodontic therapy must be performed 2 weeks after initial treatment.
6. Periodontal disease, stage 4
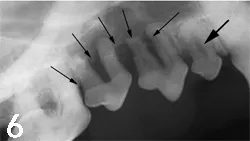
The arrows on this intraoral radiograph demonstrate alveolar bone loss (periodontitis) extending from the mesial root of the right maxillary second premolar tooth (#106) to the mesiobuccal and mesiopalatal roots of the right maxillary fourth premolar tooth (#108). The radiograph reveals stage 4 periodontal disease (greater than 50% attachment loss) of the upper right second and third premolar teeth. Root resorption is present on the mesial and distal root of the second premolar. In most cases the treatment for stage 4 periodontal disease is extraction of the affected teeth. The arrowhead points out the widened root canal of the right maxillary first molar tooth (#105), which was an incidental finding.

7. Dental caries
This gross image of the maxilla shows portions of the crown missing from the left maxillary first and second molar teeth (#109 and #110, respectively). Lesions are diagnosed in the clinical setting by the use of a dental explorer; it "sticks" in the soft decaying dentin. Carious lesions result from microbiologic activity on the occlusal surface of teeth: carbohydrates ferment and cause acid production, then acid demineralizes and destroys tooth structures. The most commonly affected teeth are maxillary first molars and mandibular first and second molars. Removal of decayed tissue allows restoration of tooth structure. However, if dental caries progresses into the pulp cavity, endodontic therapy will be required prior to restoration. In severe cases with extensive loss of dental structure, extraction will be required.

8. Class II malocclusion
This intraoral view shows a class II malocclusion, which is diagnosed when mandibular brachygnathism or maxillary prognathism is present. The gross image demonstrates the left mandibular canine tooth (#304) occluding on the palatal side of the left maxillary canine tooth (#204). In this case a mucosal draining tract located on the mucogingival line developed secondary to periodontal disease. In cases of class II malocclusions, where 1 or both mandibular canine teeth traumatically occlude with the hard palate, great potential exists for oral discomfort and formation of deep periodontal pockets (where the mandibular canine tooth contacts the hard palate). Treatment options for teeth that are in traumatic malocclusion with hard or soft tissue are orthodontic movement, partial crown amputation with vital pulpotomy and pulp capping, or extraction.

9. Dental abrasion
This photograph demonstrates severe dental abrasion on the distal surface of the left mandibular canine tooth (#304). Dental abrasion is defined as wear on the tooth surface that is not caused by occlusal contact with another tooth; it occurs on the occlusal surface of teeth or on the distal surface of the maxillary and mandibular canine teeth. In this case, the dental abrasion was caused by chewing on a metal cage. Treatment for dental abrasion secondary to cage chewing is discontinuing use of the cage and tooth restoration with a three quarter or full metal crown. If the pulp tissue is exposed, endodontic therapy will be required prior to restoration; otherwise the tooth should be extracted. Behavioral counseling should be included in the treatment plan if the patient is chewing on its cage due to separation anxiety.