Canine Lung Lobe Torsion
Christian Latimer, DVM, CCRP, DACVS-SA, Carolina Veterinary Specialists, Huntersville, North Carolina
Adesola Odunayo, DVM, MS, DACVECC, University of Florida

FIGURE 1 Intraoperative image of a congested, torsed lung lobe. Affected lung tissue is often necrotic and friable. Courtesy of Dr. Karen Tobias, University of Tennessee College of Veterinary Medicine
Lung lobe torsion (LLT) occurs when a lung lobe rotates along its long axis, causing constriction of the bronchus and vessels at the hilus (Figure 1). This life-threatening disorder requires immediate surgical intervention.
Overview
LLT occurs spontaneously or secondary to a predisposing condition, such as chylothorax, pleural effusion, or chronic respiratory disease. LLT’s pathophysiology is poorly understood but may involve partial collapse of a lung lobe, either spontaneously or secondary to disease, that leads to altered spatial association and increased relative lung mobility.1 Large, deep-chested dog breeds have a higher incidence of LLT than small-breed dogs; however, pugs may be predisposed.1 Right middle and left cranial lung lobes are most commonly affected.2,3 Median age is 3 years, although LLT has been reported in a 7-week-old pug.3,4
Clinical Signs
Dogs present acutely or chronically. Clinical signs may include tachypnea, dyspnea, and coughing with or without hemoptysis. Dogs with concomitant pleural effusion may present in respiratory distress. Anorexia, weight loss, and vomiting are seen in chronic cases.
Diagnosis
Thoracic radiographs (Figures 2–3) usually show pleural effusion and an opacified lung lobe. In acute cases, there may be an alveolar pattern in the affected lung lobe. A vesicular pattern (small, scattered gas bubbles) in the affected lung lobe; mediastinal shift; axial rotation of the carina; abnormal orientation of the bronchi in the affected lung lobe; and a curved, dorsally displaced trachea are common radiographic findings.2,5
Computed tomography (CT), thoracic ultrasound, and bronchoscopy may be helpful when thoracic radiographs are not diagnostic. CT images (Figure 4) show abruptly ending lobar bronchus of the affected lobe and noncontrast enhancing lung lobe enlargement in addition to pleural effusion and vesicular emphysema.5,6 The torsed lung appears rounded, hypoechoic, and surrounded by pleural effusion on ultrasonography.5 Definitive diagnosis is made by direct inspection at surgery or necropsy.
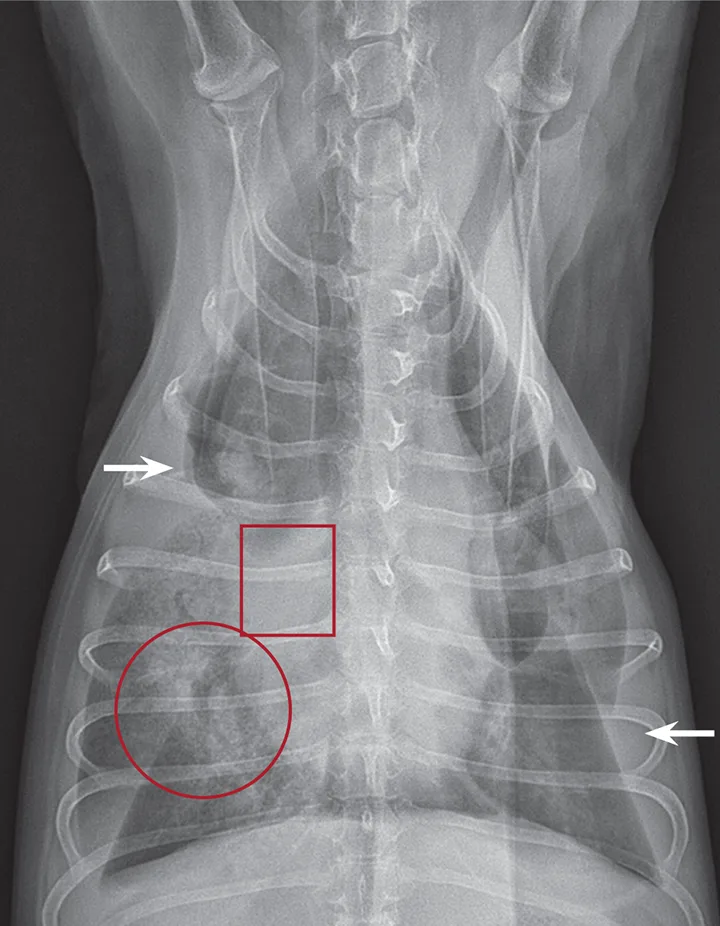
Figure 2
Ventrodorsal thoracic radiograph of a dog with right middle LLT. There is a vesicular gas pattern and alveolar pattern throughout the right middle lung lobe (circle), and the right middle lobar bronchus abruptly truncates near the hilus (rectangle). There is a moderate volume of pleural effusion evenly distributed within the pleural space, with moderate retraction of all lung lobes away from the thoracic wall (arrows).
Treatment
LLT treatment involves surgical resection of the affected lobe. Medical management before surgery is aimed at stabilization (eg, supplemental oxygen, analgesia, thoracocentesis [if pleural effusion is present]) and treatment for underlying conditions (eg, antibiotics for pneumonia).
In surgery, the torsed lobe is approached through a lateral intercostal thoracotomy, and is removed via a stapling device. If stapling equipment is not available, the pedicle of the affected lobe is clamped, the lobe is detorsed, and the vessels and bronchus are ligated with sutures. Thoracoscopy may also be used for surgical exploration and lung lobectomy.
Prognosis
Prognosis is generally good for patients with spontaneous LLT but can be poor for those that have LLT associated with other intrathoracic pathology, such as chylothorax.
The authors would like to thank Silke Hecht, Dr. Med. Vet., DACVR, DECVDI, for her assistance with the manuscript.