Canine Glomerulonephritis
Profile
DEFINITIONGlomerulonephritis is often defined as the presence of intraglomerular immune complexes. Leakage of plasma proteins into the glomerular filtrate occurs in this disorder because of alterations in the selective permeability of the glomerular capillary wall. The term glomerulonephritis suggests associated inflammation; however, in many cases inflammatory cells are absent. Glomerular capillary wall disease may also be caused by mechanical (e.g., systemic and intraglomerular hypertension) or structural (e.g., associated with familial nephropathy in Samoyeds and glomerular amyloidosis) abnormalities.
SystemsRenal/Urologic. Proteinuria is the initial hallmark clinicopathologic finding. Glomerulonephritis can be progressive, resulting in nephron loss and renal insufficiency/failure.
Cardiovascular. With severe proteinuria leading to the nephrotic syndrome, hypoalbuminemia, edema/ascites, hypercholesterolemia, systemic hypertension, hypercoagulability, and thromboembolic disease are often present.
Genetic implicationsFamilial glomerular disease has been documented in several breeds including beagles, Bernese mountain dogs, bull terriers, English cocker spaniels, English foxhounds, dalmatians, Doberman pinschers, greyhounds, Newfoundland terriers, rottweilers, Samoyeds, and soft-coated wheaten terriers.
Incidence/PrevalenceStudies of random source dogs have demonstrated glomerulonephritis prevalence rates of 40% to 90%.
Geographic DistributionWorldwide
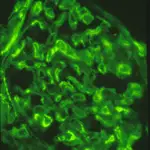
Immunofluorescent photomicrograph of a glomerulus from a dog with immune complex glomerulonephritis (stained with fluorescent antibody directed against canine IgG)
SIGNALMENTBreed predilection. See genetic implications above. In addition to breeds at risk for familial disease, golden and Labrador retrievers, long-haired dachshunds, and miniature schnauzers appear to be overrepresented in some retrospective studies. Golden and Labrador retrievers may also be predisposed to developing Lyme disease-associated glomerulonephritis.
Age and range. Mean age for dogs diagnosed with immune-complex glomerulonephritis is 6.5 to 7.0 years. Familial glomerular disease may manifest at an early age (< 1 year).
Gender. No gender predisposition has been observed for immune-complex glomerulopathy in dogs. Familial glomerular disease may have a gender predisposition (e.g., X-linked hereditary nephropathy of male Samoyeds and English cocker spaniels).
CAUSES/RISK FACTORSAntibody response against normal glomerular capillary walls (autoimmune disease) has not been documented in dogs. Several infectious and inflammatory diseases have been associated with immune-complex glomerulonephritis (Table); however, in many cases an antigen source or underlying disease is not identified and glomerulonephritis is referred to as idiopathic.
PATHOPHYSIOLOGY/CLINICAL SIGNSAntigen-antibody complexes may be deposited or trapped within the glomerulus or they may form in situ. In situ immune complex formation occurs when circulating antibody reacts with antigen that has been incorporated or "planted" in the glomerular capillary wall. Subsequent to formation or deposition of glomerular immune complexes, a cascade of events is often triggered that results in glomerular damage and proteinuria. For example, activation of complement; platelet aggregation; and production of cytokines, growth factors, and eicosanoids can damage the glomerulus and alter its permselectivity resulting in proteinuria. In some cases of familial nephropathy, there are structural abnormalities in basement membrane collagen that result in proteinuria. The glomerulus responds to these various insults by cellular proliferation (proliferative glomerulonephritis), thickening of the capillary walls (membranous glomerulonephritis), and if the injury is persistent and severe, sclerotic changes that can lead to loss of the entire nephron. It is interesting to note that an abnormal amount of protein in the glomerular filtrate is not just a diagnostic marker but may also cause disease progression in the form of glomerular and tubulointerstitial damage.
DiagnosisHistory/physical examinationWith mild to moderate proteinuria, historical and physical findings may be absent or include such nonspecific signs as mild weight loss, decreased muscle mass, and lack of stamina. Proteinuria and/or microalbuminuria is often discovered during annual wellness examinations. In some cases, proteinuria is observed in dogs presented because of an underlying infectious or inflammatory disease process. If protein loss is severe (serum albumin concentrations < 1.5 to 1.0 g/dl), peripheral edema and/or ascites is often present. If glomerular disease progresses to renal insufficiency or failure; polydipsia, polyuria, anorexia, nausea, vomiting, and more severe weight loss may be observed along with azotemia, hyperphosphatemia, anemia, and decreased urine concentration. Acute dyspnea may be caused by pulmonary thromboembolism (rare), and acute blindness associated with systemic hypertension may be caused by retinal hemorrhage or detachment (rare).
ImagingSpecific changes are usually not noted on abdominal radiographs or ultrasonography. Imaging of the thorax and abdomen can help rule in or out underlying disease processes. Renal biopsy specimens can be obtained percutaneously with ultrasonographic guidance.
Laboratory findingsProteinuria is the hallmark clinicopathologic abnormality of glomerulonephritis. Glomerular proteinuria is persistent and usually associated with normal or inactive urine sediment, although hyaline casts may be observed. Probably the most common cause of proteinuria in dogs is inflammation of the lower urinary tract, which can usually be diagnosed on the basis of an active urine sediment (e.g., bacteriuria and increased numbers of white and red blood cells and epithelial cells per high-power field). The urine protein-creatinine ratio (UP/C) is used to quantitate and confirm increased urine protein concentrations when proteinuria is believed to be glomerular in origin. Since the magnitude of the proteinuria roughly approximates the severity of the glomerular lesions, the UP/C can be useful in assessing disease progression and response to therapy. Hypoalbuminemia and hypercholesterolemia are common serum biochemistry findings in cases of moderate to severe glomerular proteinuria. Recent evidence suggests that persistent microalbuminuria is a valuable tool for early diagnosis of glomerular disease. Single positive tests should be followed up with retesting as transient microalbuminuria may be clinically insignificant.
Definitive diagnosisHistopathologic evaluation of the renal cortex not only provides a definitive diagnosis but also provides valuable prognostic information. Renal biopsy should be done only after the patient has been thoroughly evaluated for any underlying disease process and platelet numbers and blood clotting ability have been assessed.
Photomicrograph of a hyaline cast from the urine sediment of a dog with protein-losing nephropahty.
TreatmentSince most glomerulonephritis is associated with immune-mediated disease, often the best treatment is to identify and correct the underlying source of antigenic stimulation. In many cases, however, the underlying disease process cannot be identified or is impossible to eliminate (e.g., neoplasia). Immunosuppressive drugs are generally ineffective except in cases where the underlying disease process is responsive to immunosuppression (e.g., immune-mediated hemolytic anemia, systemic lupus erythematosus). Low-dose aspirin treatment (0.5 mg/kg Q 12 H) has been recommended for antiinflammatory and antiplatelet effects. Angiotensin-converting enzyme inhibitors (ACEIs) (e.g., enalapril, 0.5 mg/kg Q 12 to 24 H) have generally been effective in reducing systemic hypertension and proteinuria and slowing disease progression in dogs with idiopathic glomerulonephritis. In addition, sodium-reduced, high-quality, low-protein diets are often recommended for dogs with protein-losing nephropathies (e.g., early renal failure prescription diets).
In General
RELATIVE COST OF TREATMENTThe "antigen hunt" portion of the workup is often the most expensive. A minimum database, thoracic radiographs, abdominal radiographs or ultrasonography, antinuclear antibody titers, infectious disease serologic testing (e.g., heartworm, Ehrlichia, and Lyme disease) and blood pressure assessment can cost more than $500 in many parts of the country. Obtaining a renal biopsy with histologic assessment by light, immunocytochemical, and electron microscopy may cost $200 to $300. The cost of long-term treatment with ACEIs varies depending on the size of the dog, and routine follow-up examinations may cost as much as $100 to $150.
FUTURE CONSIDERATIONSAs our profession performs more renal biopsies in dogs with glomerular disease, it is likely that specific treatment recommendations will emerge for the different histologic forms of the disease. Similarly, as more data on microalbuminuria in dogs surface, it is likely that testing for microalbuminuria will become a routine and important diagnostic tool for early renal disease.
Follow-up
Patient monitoringThe UP/C should be followed closely in animals with glomerulonephritis to assess response to treatment and/or progression of disease. A favorable response to either correction of an underlying disorder or ACEI treatment of idiopathic glomerulonephritis would be a 50% reduction in the UP/C in conjunction with a stable or declining serum creatinine concentration. Blood pressure should also be routinely monitored. Ideally, patients should be rechecked at 1, 3, 6, 9, and 12 months after the start of treatment.
PrognosisThe outcome of glomerulonephritis varies. Glomerular disease can be self-limiting and reversible. In some cases, ACEI treatment can improve, stabilize, or at least retard the progressive nature of the disease. In other cases, the disease will progress to chronic renal insufficiency/failure despite treatment.
Diseases Associated with Glomerulonephritis in Dogs
InfectiousCanine adenovirus IBacterial endocarditisBrucellosisHeartworm diseaseEhrlichiosisLeishmaniasisPyometraBorelliosisChronic bacterial infections (gingivitis, pyoderma)Rocky Mountain spotted feverTrypanosomiasisSepticemiaHelicobacter?
Neoplastic
All types
InflammatoryPancreatitisSystemic lupus erythematosusOther immune-mediated diseasesProstatitisHepatitisInflammatory bowel disease
OtherHyperadrenocorticism and administration of long-term high-dose corticosteroidsIdiopathicFamilialNonimmunologic-hyperfiltrationDiabetes mellitus
TX at a glance
Identify/correct underlying source of antigenic stimulation, if possible.
Administer immunosuppressive drugs only if underlying disease process is responsive to immunosuppression (e.g., immune-mediated hemolytic anemia or systemic lupus erythematosus).
Give low-dose aspirin (0.5 mg/kg Q 12 H) for antiinflammatory and antiplatelet effects. Use angiotensin-converting enzyme inhibitors (e.g., enalapril, 0.5 mg/kg Q 12 to 24 H) for reducing systemic and intraglomerular hypertension and proteinuria and slowing disease progression in cases.
Encourage owners to feed a sodium-reduced, high-quality, low-protein diet if dog has protein-losing nephropathy.
GLOMERULAR DISEASE • Gregory F. Grauer
Suggested ReadingClinicopathologic, renal immunofluorescent, and light microscopic features of glomerulonephritis in the dog: 41 cases (1975-1985). Center SA, Smith CA, Wilkinson E, et al. JAVMA 190:81, 1987.Clinical and pathological features of protein-losing glomerular disease in the dog: a review of 137 cases (1985-1992). Cook AK, Cowgill LD. JAAHA 32:313, 1996.Morphologic, immunohistochemical, and ultrastructural characterization of a distinctive renal lesion in dogs putatively associated with Borrelia burgdorferi infection: 49 cases (1987-1992). Dambach DM, Smith CA, Lewis RM, et al. Vet Pathol 34:85, 1997.Glomerulonephritis. Grauer GF. Semin Vet Med Surg (Small Anim) 7:187, 1992.Glomerular disease. Grauer GF, DiBartola SP. In: Ettinger SJ, Feldman EC (eds): Textbook of Veterinary Internal Medicine, ed 4. Philadelphia: WB Saunders, 2000.Effects of enalapril versus placebo as a treatment for canine idiopathic glomerulonephritis. Grauer GF, Greco DS, Getzy DM, et al. J Vet Intern Med 14:526, 2000.Hypercoagulable state in three dogs with nephrotic syndrome: role of acquired antithrombin III deficiency. Green RA, Kabel AL. JAVMA 181:914, 1982.Hypoalbuminemia-related platelet hypersensitivity in two dogs with nephrotic syndrome. Green RA, Russo EA, Greene RT, et al. JAVMA 186:485, 1985.Treatment of X-linked hereditary nephritis in Samoyed dogs with angiotensin converting enzyme (ACE) inhibitor. Grodecki KM, Gains MJ, Baumal R, et al. J Comp Pathol 117:209, 1997.
Membranous nephropathy in the dog. Jaenke RS, Allen TA. Vet Pathol 23:718, 1986.Canine chronic renal disease: prevalence and types of glomerulonephritis in the dog. MacDougall DF, Cook T, Steward AP, et al. Kidney Int 29:144, 1986.Nephrotic syndrome in dogs: diagnosis and treatment. Relford RL, Lees GE. Compend Contin Educ Pract Vet 18:279, 1996.The effects of cyclosporin versus standard care in dogs with naturally occurring glomerulonephritis. Vaden SL, Breitschwerdt EB, Armstrong PJ, et al. J Vet Intern Med 9:259, 1995.