Canine Cesarean Section
Youry Dupré, DVM, Animal Surgical Center of Michigan, Flint, Michigan
W. Alex Fox-Alvarez, DVM, MS, DACVS-SA, Community Care Veterinary Specialists, Gainesville, Florida

Successful management of dystocia requires thorough evaluation, diagnostic investigation, and medical treatment when safe and appropriate. Medical management is successful in ≈40% of dogs with dystocia.1-3 Oxytocin and calcium gluconate are often used to help with uterine contractions but are not always successful. Cesarean section is the treatment of choice if medical management fails or is contraindicated or if there are signs of fetal distress or maternal exhaustion (see Situations When Cesarean Section Is Indicated).
SITUATIONS WHEN CESAREAN SECTION IS INDICATED
Pelvic canal obstruction
Fetal–maternal size disparity
Fetal malposition
Previous pelvic fracture malunion
Vaginal stricture or canal obstruction
Predisposed breed (eg, brachycephalic breeds)
Fetal considerations
Bradycardia (<180 bpm)
Asystole
Maternal considerations
Primary uterine inertia nonresponsive to medical management
Uterine rupture
Lochia present >4 hours
Strong contractions for >30 minutes without fetal expulsion (secondary uterine inertia)
>4 fetuses remain after attempted medical management
Evidence of systemic illness in the dam
Although the decision on whether a cesarean section is needed must be made quickly, pet owners should be counseled on the possibility of complications, including death of one or more fetuses and/or the dam, depending on the dam’s clinical status. Concurrent ovariohysterectomy should also be discussed as both an elective and a potentially necessary treatment if uterine pathology is identified during surgery.
Preoperative Preparation
Coordination of surgical, anesthetic, and nursing teams is key for speed and efficiency. These roles may overlap, making it especially important to establish and communicate who is responsible for each element of the care plan. A preoperative checklist can be helpful in emergency surgeries to minimize oversight that could harm the patient or increase anesthetic duration. Because prolonged anesthesia times have been inconsistently associated with an increase in perinatal death,4,5 the pace of emergency surgery should not be frantic. Surgery should, however, be performed as quickly as possible to minimize anesthetic exposure to the fetus(es) without sacrificing the safety and comfort of the dam. Preoperative injectable pain medication is typically not administered, as it could affect neonatal recovery, but can be used intraoperatively after fetus removal.
If temperament allows, the dam should ideally be awake for catheter placement, fur clipping, and initial sterile preparation of the abdomen. Oxygen should be administered via facemask during initial preparations. Induction should take place inside the operating room to decrease the time of fetal exposure to inhalant anesthetics. The surgeon should be scrubbed and gowned prior to induction so the procedure can begin immediately following final sterile preparation of the abdomen.
An incisional line block using bupivacaine can help decrease the minimum alveolar concentration required for anesthesia maintenance. Positioning the patient in dorsal recumbency provides the best visualization and access to the dam’s reproductive system. Lateral tilting does not improve cardiovascular parameters and is not necessary.6
Anesthesia time can be further decreased by using a fast-acting, paint-on surgical preparation solution; strategically organizing the instrument table; and precutting the drapes.
Procedure
Uterotomy incision(s) should be performed in a relatively avascular area of the uterine body or the greater curvature of the uterine horn(s). Incision sites are determined based on the location and number of fetuses, number of surgeons, and uterine vascular anatomy. Up to 3 fetuses may be gently manipulated from the horns out of a single uterine body incision. If more than one fetus occupies a single horn, or if 2 surgeons are available to simultaneously remove fetuses from each horn, uterotomy at the greater curvature of the uterine horn(s) can facilitate faster removal of fetuses and thereby decrease anesthetic exposure; however, multiple incisions likely increase surgical time. The uterotomy incision should be initiated using a #15 blade and completed using Metzenbaum scissors.
Uterine tissue should be elevated from the fetuses using Debakey forceps to prevent inadvertent fetal trauma. Uterotomy incisions should be large enough to remove the fetuses without tearing the incision edges.
With gentle pressure and traction, each fetus can be removed from the uterotomy incision(s). The amniotic sac should be ruptured using blunt digital dissection. The umbilical cord should be double-clamped using mosquito forceps and incised between the 2 forceps using a scalpel blade or Metzenbaum scissors. The neonate can be wrapped in a sterile huck towel and handed to the recovery team for care and resuscitation. This process should be repeated until all neonates have been delivered. In cases of in-term or near-term dystocia, placentae peel away from the endometrium with minimal force and hemorrhage. In preterm dams, however, placentae may be more firmly fixed to the endometrium and may demonstrate significant hemorrhage on removal; in these cases, placentae can be left in place for natural expulsion or resorption.
After neonates have been removed, a single dose of an opioid analgesia for pain may be administered to the dam if the drug was not administered preoperatively (see Preoperative Preparation).
Postoperative Care
Neonate Recovery
While the surgical team delivers the neonates and transitions to closure of the dam, the recovery team provides care to the newborn puppies. Each neonate should be rubbed vigorously with a towel until respiration is noted, and a suction bulb can be used to remove fluid from the upper respiratory tract (ie, mouth, nostrils, nasal cavity, pharynx; Figure 1). Swinging neonates is not recommended, as this may cause injury.
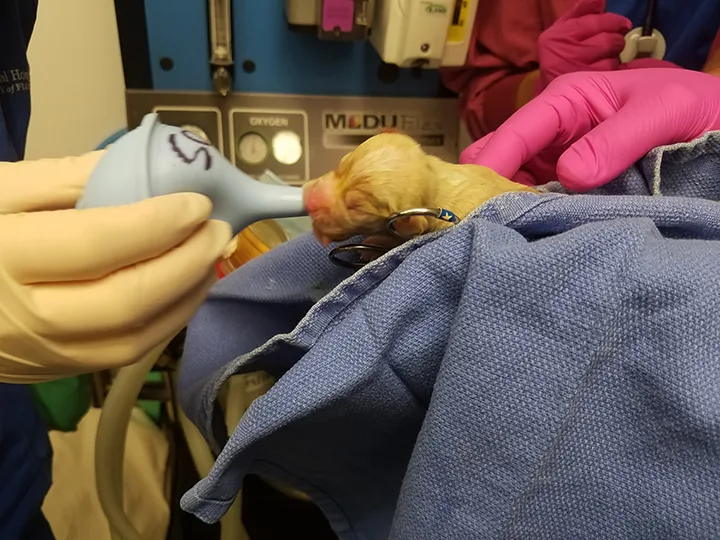
A clean suction bulb is used to remove fluid from the upper respiratory tract.
Neonates should be evaluated for activity, muscle tone, heart rate, respiratory rate, mucous membrane color, and congenital abnormalities (eg, cleft palate, atresia ani). The umbilical cord should be ligated 1 to 2 cm from the abdominal wall using absorbable suture (Figure 2).

The umbilical cord is ligated 1 to 2 cm from the abdominal wall using absorbable suture.
Closure
Uterotomy sites should be closed using a 3-0 or 4-0 monofilament absorbable suture in a single-layer continuous appositional or inverting pattern (eg, Cushing, Lembert) or using a 2-layer closure with the second layer inverting the first. Myometrium and submucosa should be included in the closure, and luminal penetration should be avoided.
After uterine closure, local lavage should be performed with sterile saline while the uterus is still isolated from the abdominal cavity with sponges. This can be followed by abdominal lavage using warm sterile saline (100-200 mL/kg). Limited abdominal exploratory should be performed to ensure no other pathology is present. Sponges and hemostats need to be counted prior to abdominal closure to prevent retained foreign material.
Abdominal closure is routine. An intradermal skin closure pattern (Figure 3) is ideal to prevent milk or fecal debris from encrusting on suture tags, as puppies will be active in the area of the incision when nursing. An impermeable bandage can be used to protect the incision from contamination during nursing. If a line block was not performed prior to surgery, it can be completed at closure, or a transversus abdominis plane block can be performed with ultrasound guidance prior to recovery to minimize the need for opioid analgesics.

Intradermal closure after cesarean section. The incision encompasses most of the caudal two-thirds of the ventral abdomen to facilitate adequate exposure of the gravid reproductive tract. An intradermal skin closure pattern is ideal to protect the incision from activity during nursing.
The dam should be recovered quickly to facilitate early nursing and maternal bonding. Close observation is needed after initial introduction of the puppies to ensure the dam is adequately recovered and receptive. This can help prevent inadvertent or intentional maternal injury to the puppies. After the neonates and dam are stable, they should ideally be returned to their home environment to reduce stress.
Maternal pain can be managed with a single postoperative dose of an NSAID (eg, meloxicam, 0.1 mg/kg IV) and an opioid analgesic (eg, methadone, 0.05-0.2 mg/kg IV every 4-6 hours) as needed for pain.7 Limited research has been done on the effect of pain medication on nursing dams and their puppies, although it is estimated that 1% to 2% of the maternal dose reaches the neonates.7 Repeat doses of NSAIDs should be avoided to minimize exposure to the developing neonatal kidneys.
Use of opioids that are less lipophilic (eg, morphine, hydromorphone, methadone) as needed after pain scoring the dam will decrease neonatal exposure.7 Neonatal adverse reactions to opioid exposure can be minimized via nursing immediately prior to opioid administration, active surveillance of neonatal behavior for respiratory depression and lack of vigor, and intervening with naloxone (1 drop of 0.4 mg/mL formulation under the tongue) to reverse any adverse effects.
Antibiotics are not necessary after uncomplicated cesarean section. When antibiotics are indicated (eg, mastitis, metritis), beta lactams (eg, ampicillin, cephalexin, amoxicillin ± clavulanate) are most often used.8
Step-by-Step: Cesarean Section
WHAT YOU WILL NEED
Standard surgical pack
Minimum 2 hemostatic forceps per neonate
Sterile towels (4) for draping, plus one additional towel per neonate
Suture material (3-0 or 4-0 monofilament absorbable suture) on a taper needle for uterine closure; standard absorbable suture material (0 and/or 2-0) on a reverse-cutting needle for abdominal closure
Sterile saline or balanced lavage solution
Step 1
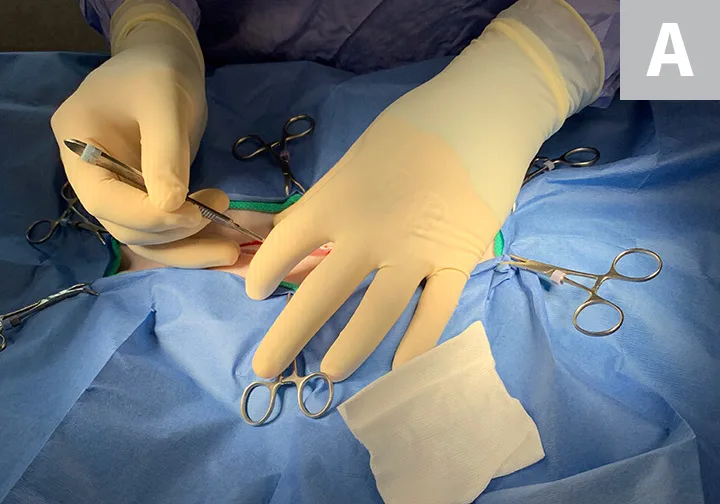
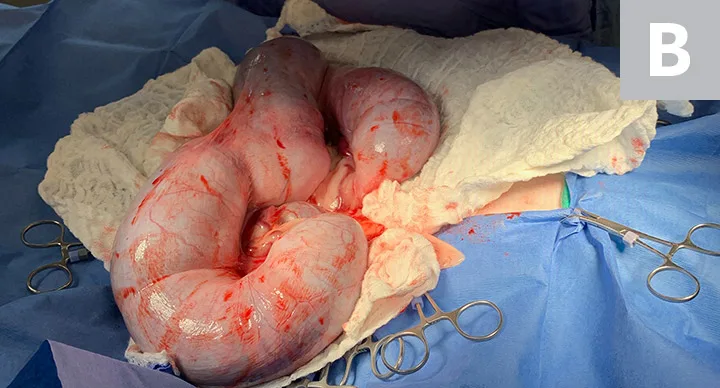
With the patient in dorsal recumbency, anesthetize the patient, then towel and drape the entire abdomen from xiphoid to pubis to allow extension of the incision as needed. Make an incision spanning the caudal two-thirds of the abdomen just cranial to the pubis to facilitate gentle and efficient exteriorization of the uterus (A). Use Adson forceps to elevate the gravid uterus and access the abdomen. Carefully exteriorize and isolate the uterus with moist sterile laparotomy pads (B).
Author Insight
To avoid inadvertent rupture of the gravid uterus, keep fingers together and use the entire hand in a scooping motion to manipulate the uterine horns out of the abdomen.
Step 2
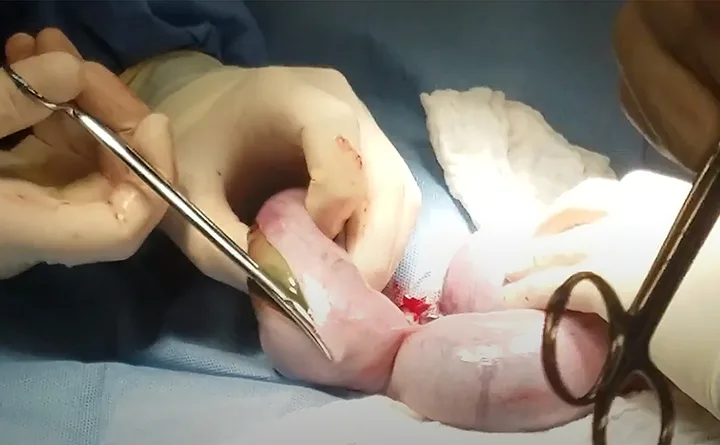
Use Debakey forceps to elevate the uterine wall away from the underlying fetuses. Using a #15 blade, make a uterotomy incision at the predetermined site; finish the incision with Metzenbaum scissors. Repeat at other sites in the opposite uterine horn or body as needed.
Step 3
Once the uterus is incised, use gentle pressure and traction to remove each fetus from the uterotomy incision(s). Use blunt digital dissection to rupture the amniotic sac. Double clamp the umbilical cord with mosquito forceps, and then incise it between the forceps using a scalpel blade or Metzenbaum scissors. Pass each neonate in a sterile huck towel to the recovery team for care and resuscitation. Repeat this process until all neonates have been delivered.

Step 4
Close uterotomy sites using a 3-0 or 4-0 monofilament absorbable suture in a single-layer continuous appositional or inverting pattern or with a 2-layer closure with the second layer inverting the first. Include the myometrium and submucosa and avoid luminal penetration. Change heavily soiled gloves. With the uterus still isolated from the abdomen, perform local lavage and subsequent abdominal lavage with sterile saline. Perform a limited abdominal exploratory to ensure no abnormalities are present, and then perform routine abdominal closure.