Overview
Bartonella spp are emerging zoonotic, intraerythrocytic, endotheliotropic bacteria of increasing importance in veterinary and human medicine.1-3 These bacteria have been associated with a spectrum of disease manifestations involving the lymph nodes, heart (valves and myocardium), vasculature, liver, spleen, joints, and CNS.4 Approximately 20 Bartonella spp have been identified as pathogenic for human disease, and 6 of these have been isolated from pet cats and dogs.1 Bartonella henselae and Bartonella vinsonii subspecies berkhoffii are the most often identified species in sick dogs and have been isolated from the blood of immunocompetent humans.4
Epidemiology
Geographic Distribution
Distribution varies greatly, likely reflecting the distribution of hosts and vectors.
Prevalence is higher in regions where flea and tick infestations are more likely.1,2,5
B henselae, B vinsonii subspecies berkhoffii, and Bartonella koehlerae have worldwide distributions.
Based on seroprevalence data, dogs are exposed to B henselae, B vinsonii subspecies berkhoffii, and B koehlerae throughout the United States, but some research has demonstrated that B vinsonii seropositivity may be more likely in tropical and coastal areas with high levels of precipitation (Figures 1-3).1,2,6
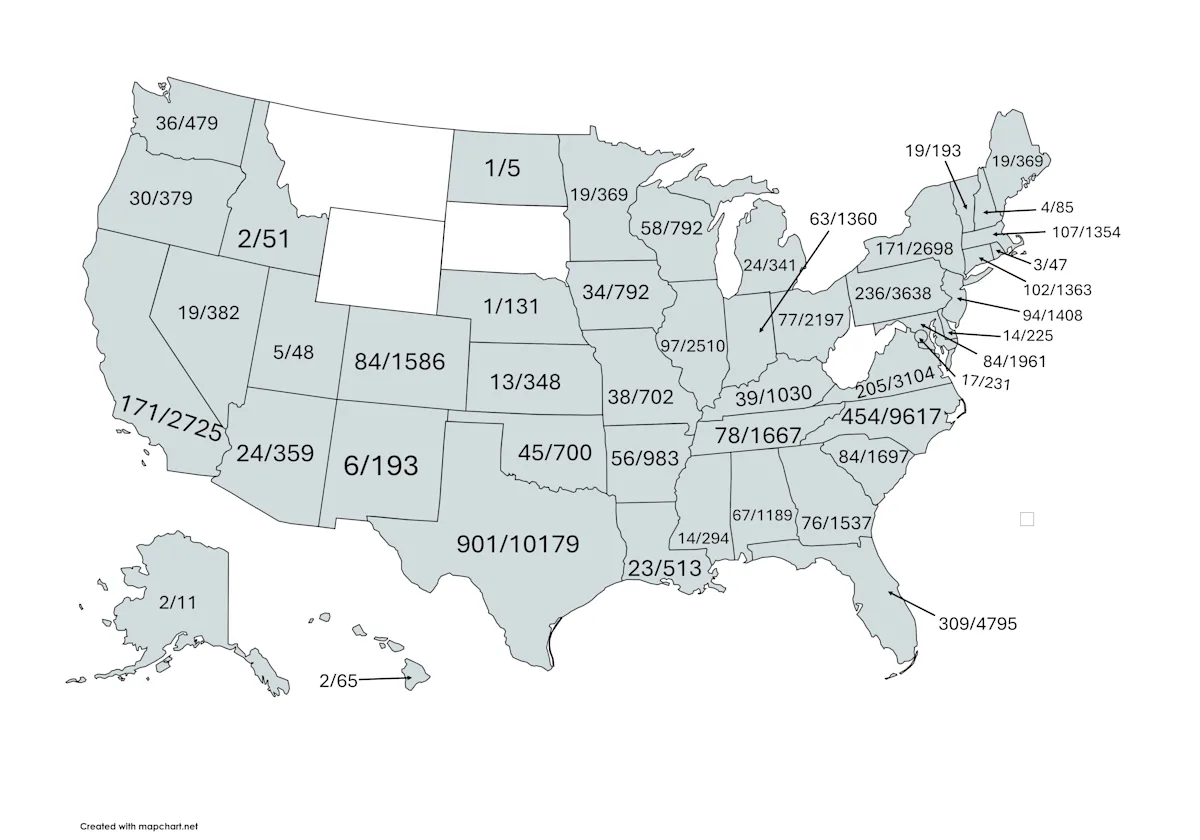
FIGURE 1
B henselae seroprevalence by state for dogs tested between March 2008 and July 2024 at North Carolina State University College of Veterinary Medicine, Vector-Borne Diseases Diagnostic Laboratory. An antibody titer of 1:64 was considered seroreactive.
Incidence/Prevalence
Cats are the primary reservoir host for B henselae and B koehlerae.
Transmission among cats, and potentially dogs, occurs via flea bites or scratch inoculation of flea feces.
Canids (eg, coyotes, dogs, gray foxes) can serve as reservoir hosts for B vinsonii subspecies berkhoffii.
Tick transmission of this subspecies is suspected.5,7
In nontropical areas, dogs appear to be accidental hosts for several Bartonella spp.1,2
Signalment
Species
B henselae, B vinsonii subspecies berkhoffii, and Bartonella rochalimae have caused endocarditis in dogs and humans.4
Seven Bartonella spp have been found to cause endocarditis in dogs.1,2
Breed Predisposition
Epidemiologically, seroprevalence of B henselae and B vinsonii subspecies berkhoffii correlates with midsize and large-breed dogs that are allowed to roam.6,8,9
Age
Exposure is more likely in middle-aged to older dogs.
Sex
Although female sex predisposition is suspected in humans,10 no sex predisposition has been identified in dogs.
Genetic Implications
Genetic predisposition may exist.
Bartonella spp have been found in 18% of healthy golden retrievers; although US data are scarce, some research suggests overall seroprevalence is <5%.1,11
In a study involving 1,872 working dogs owned by the US government, German shepherd dogs were significantly less likely to be seropositive for B vinsonii subspecies berkhoffii than other breeds.12
Causes & Risk Factors
Less is known about risk factors for canine bartonellosis, but infection is most likely via animal scratches and bites from fleas, ticks, and other arthropod vectors.
Interest in the role of tick bites in transmitting Bartonella spp infection is increasing because of some correlation found between high tick burden and B vinsonii subspecies berkhoffii seroactivity.5,7 These bacteria pose an occupational risk for animal health professionals.13,14
Exposure is more likely in dogs that live in rural environments and have frequent flea and tick exposure.15
Acquired or therapeutically induced immunosuppression enhances disease expression. Reactivation of occult Bartonella sppinfection can occur in association with severe illnesses caused by other infections, traumatic events, and/or stress.
Pathophysiology
Presumably complex, the pathophysiology of Bartonella spp infection is incompletely understood.3,4 Following transmission, bacteria localize to erythrocytes, endothelial cells, and (based on in vitro data) macrophages, as well as dendritic, microglial, and CD34 bone marrow progenitor cells.1,16,17 Lymphoid hyperplasia, granulomatous inflammation in a variety of tissues, vasculitis, thromboses, and vasoproliferative lesions are among the reported pathologic lesions.
History
Due to the highly adaptive nature of these vector borne bacteria, most dogs experience acute illness that may or may not be associated with fever or evidence of a systemic inflammatory response, followed by a chronic, insidious course of illness spanning months to years. Lameness, intermittent lethargy or fever, epistaxis, and neurologic abnormalities, including lack of coordination or seizures, can develop progressively in chronically infected dogs.4,18-20
Clinical Presentation
Chronically infected dogs may not exhibit clinical signs of illness.21
Dogs with neutrophilic polyarthritis may exhibit a mild shifting-leg lameness or severe debilitating joint pain.
Differential Diagnoses
As intravascular, endotheliotropic bacteria, Bartonella spp can localize to numerous tissue locations within the body.
Bartonellosis would be a differential diagnosis for dogs with endocarditis, myocarditis, polyarthritis, meningoencephalitis, granulomatous inflammatory disease, lymphoid hyperplasia, hypersplenism, epistaxis, idiopathic cavitary effusions, vasculitis, thrombosis, fever of unknown origin, or vasoproliferative lesions.
Each of these conditions can be caused by numerous infectious, neoplastic, and autoimmune conditions. Due to the presence of antinuclear antibodies in dogs with bartonellosis, infection with these bacteria should be ruled out in dogs with suspected systemic lupus erythematosus.
Diagnostics & Diagnostic Findings
Definitive Diagnosis
As with other intracellular pathogens that induce chronic infection in dogs after vector-borne transmission, diagnostic confirmation of active infection with a Bartonella spp can be extremely challenging.
Because of the cost and duration of therapy, a diagnosis of bartonellosis should be confirmed by culturing the organism from blood; cerebrospinal, aqueous, or joint fluids; thoracic, pericardial, or abdominal effusions; or tissue biopsy samples.
Fresh or frozen samples can be used for cultivation of Bartonella spp.
PCR Assay
When using agar plates for blood culture in cats, B henselae and Bartonella clarridgeae can often be readily isolated; however, isolation from dog, horse, or human blood samples using the same approach is highly insensitive.22
To increase diagnostic sensitivity, enrichment culture in a specialized growth medium (designated Bartonella alpha–Proteobacteria growth medium [BAPGM]) was combined with a highly sensitive PCR assay.
Currently, BAPGM enrichment blood culture provides the most sensitive (98% at 1 bacterium/mcL) modality to confirm active Bartonella spp infection in companion animal or human blood specimens (Figure 4).22,23
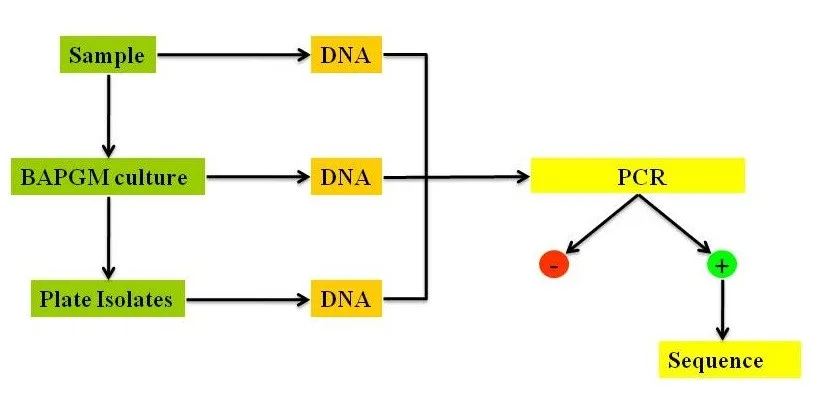
Diagram depicting the steps involved in the BAPGM platform. PCR is performed following extraction of DNA from the original patient sample, enrichment incubation in BAPGM, and subculture onto a blood agar plate. BAPGM is an insect cell culture–based liquid growth medium optimized to facilitate growth of Bartonella spp and other fastidious bacteria.22 The enrichment process increases the quantity of Bartonella spp DNA to enhance the sensitivity of the PCR assay. PCR-positive samples are sequenced to determine the Bartonella spp and strain.
Alternatively, PCR can be used to amplify Bartonella spp DNA from fresh frozen or formalin-fixed paraffin-embedded (FFPE) lymph nodes, heart valves, or other tissues, but PCR following enrichment culture is reportedly 2 to 3 times more sensitive than direct PCR alone.24,25
PCR from fresh frozen biopsy or necropsy tissues is more sensitive than PCR from FFPE tissues.
Immunosuppressive drugs appear to increase the quantity of Bartonella spp in blood, whereas administration of antibiotics prior to obtaining samples for BAPGM culture decreases detection via culture or PCR.
IFA Testing
Indirect immunofluorescent antibody (IFA) testing using canine sera is highly specific (≥97% specificity).6,26,27
However, antibody reactivity to Bartonella spp antigens is detected in only 50% of dogs and humans in which active infection with B vinsonii subspecies berkhoffii and B henselae DNA can be documented (Figure 5).6,26,27
IFA antibody testing in dogs and humans is therefore insensitive; however, if seroreactive, the presence of antibodies infers prior exposure.4
With the exception of Bartonella spp-induced endocarditis, IFA antibody titers in sick dogs are often low.
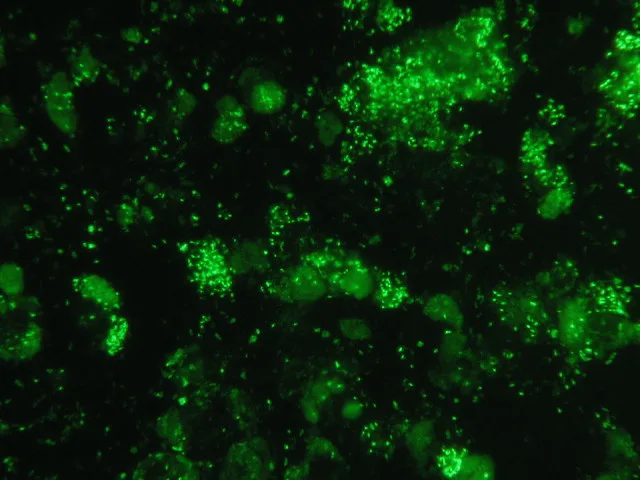
B vinsonii subspecies berkhoffii immunofluorescent organisms (serum antibody titer of 1:2,048) seen via the IFA serologic assay in the North Carolina State University Vector-Borne Diseases Diagnostic Laboratory. The test serum was from a military working dog with B vinsonii subspecies berkhoffii genotype III endocarditis. Bacteremia was confirmed using the BAPGM platform.
Other Laboratory Findings
Most dogs chronically infected with Bartonella spp have no laboratory abnormalities until fulminant clinical signs develop; laboratory abnormalities are then nonspecific.24,25,28,29
Bartonella spp have been isolated from the blood, CSF, and joint effusion samples of dogs with immune-mediated hemolytic anemia, immune-mediated thrombocytopenia, neutropenia, neutrophilia with a mild left shift, eosinophilia, unexplained hypoalbuminemia, mild hyperglobulinemia, mild to moderate elevations in liver enzyme activities, or hematuria.
Postmortem Findings
Bartonella spp infections are chronic. Causation has thus not been clearly established for many pathologic lesions found in culture- or PCR-positive dogs.
Multiple Bartonella spp have been associated with endocarditis in dogs.
Other pathologic lesions for which these bacteria should be considered include4,30:
Granulomatous lesions of undetermined cause
Lymphoid hyperplasia
Hypersplenism
Peliosis hepatis
Bacillary angiomatosis
Two studies have reported high prevalence of Bartonella spp DNA in dogs with hemangiosarcoma.31,32
Whether Bartonella spp infection is a cofactor or cause of hemangiosarcoma is unknown.
Whether treatment could decrease the rate of metastasis and improve survival outcomes is also unknown.
Treatment
Inpatient or Outpatient
Most dogs can be treated on an outpatient basis following diagnostic confirmation of active infection.
Dogs with severe life-threatening illness (eg, endocarditis, myocarditis, encephalitis, immune-mediated hemolytic anemia, idiopathic thrombocytopenic purpura) require IV antibiotics in conjunction with intensive monitoring and critical care.
Temporary immunosuppressive drugs may also be needed to suppress immune destruction of platelets or erythrocytes.
Long-term immunosuppression in conjunction with Bartonella spp–directed antibiotic therapy decreases antibiotic efficacy and prevents elimination of infection.
Medical
Antibiotics are currently the mainstay of treatment. Because Bartonella spp can induce intracellular as well as intravascular infection, antibiotics should be administered to achieve therapeutic drug concentrations in cells and plasma.
Antibiotics used to treat bartonellosis can induce anorexia, vomiting, diarrhea, and increased liver enzyme activities; however, most dogs tolerate administration of 2 or 3 antibiotics.
Based on in vitroantimicrobial testing, azithromycin, doxycycline, enrofloxacin, and rifampin are effective antibiotics.33
Azithromycin should be used with caution, as treatment failure has been documented, and there is evidence supporting rapid development of resistance.25,34
Doxycycline as sole therapy can induce clinical or hematologic improvement but does not eliminate infection.
Dogs are treated with antibiotics for a minimum of 6 weeks (see Treatment at a Glance).
A combination of 2 antibiotics is recommended to achieve cure.35
Addition of a third antibiotic has been used in refractory cases or in cases in which disease relapse occurs.36
Lethargy and inappetence are common 3 to 6 days after initiation of antibiotics, presumably due to bacterial death and rapid cytokine release.
Administering anti-inflammatory corticosteroids and short-duration therapy for anorexia or vomiting may resolve clinical signs and allow continuation of antibiotics.
Pain management may also be needed.
Antibiotic therapy for treatment of bartonellosis in dogs is protracted; definitive diagnosis is therefore recommended.
Alternative therapies have not eliminated this infection in dogs, and no alternative therapy has been shown to produce adjunctive effects.
Surgical
Surgery may be required in select cases to obtain tissue biopsies for histopathology, BAPGM enrichment culture, and PCR.
Activity
Moderate exercise restriction is only applicable for dogs with endocarditis, myocarditis, or severe debilitating polyarthritis.
Nutritional Concerns
Substantial unexplained weight loss has occurred in a small subset of dogs and humans in which Bartonella spp bacteremia was confirmed.1,37 Feeding a high-quality, high-quantity protein diet should enhance immune function and facilitate antibiotic elimination of infection.
Treatment at a Glance
Definitive treatment regimens have not been established for dogs.
Doxycycline (5 mg/kg PO) and enrofloxacin (5 mg/kg PO) every 12 hours for a minimum of 6 weeks36 or Doxycycline (5 mg/kg PO) and rifampin (5 mg/kg PO) every 12 hours for a minimum of 6 weeks36
Clarithromycin (7.5-10 mg/kg PO) every 12 hours may be added to one of the above regimens for refractory cases or relapses36
If endocarditis is documented, initial treatment (ie, doxycycline) can be given with an aminoglycoside (eg, amikacin) for 1-2 weeks while renal function is monitored. After 4 days, if antibiotics are well tolerated, enrofloxacin can be added. Doxycycline and enrofloxacin are typically continued for several months following cessation of the aminoglycoside.46
Must-Reads From Our Newsletter
Monitoring & Follow-Up
CBC and serum chemistry profile should be performed 2 weeks after initiation of antibiotic therapy or sooner if the dog experiences progressive clinical signs of illness.
Sequentially following indirect fluorescent antibody titers to document seroreversion to an antibody negative state—in conjunction with elimination of clinical, hematologic, or biochemical abnormalties (if present)—can be used to assess antibiotic efficacy, support the diagnosis of bartonellosis, and help determine when antibiotic therapy is no longer indicated.
To confirm therapeutic elimination of infection, a BAPGM platform culture/PCR assay should be performed 2 to 4 weeks after completion of antibiotics.
Antibody titers drop rapidly in Bartonella spp seroreactive dogs. Most successfully treated dogs become seronegative in 3 to 6 months.38,39
Complications
Treatment failures are a major complication, potentially due to treatment with a single antibiotic, duration of therapy that is too short, or current immunosuppression.
Prognosis
Prognosis varies from grave to good, depending on duration of infection, disease manifestations, and response to antibiotics.
Prevention & Owner Education
All known Bartonella spp are transmitted by a spectrum of arthropod vectors, by animal bites or scratches, by blood transfusion from an infected donor, or mechanically by needlesticks.1-5
Flea infestations should be eliminated and future infestations prevented with preventive products that repel and kill arthropod vectors.
In conjunction with directed medical therapy, pet owners should apply acaricides to prevent future vector transmission by fleas or ticks.5,8,9,11
Bites, scratches, contact with saliva, and needlesticks should be avoided.
Zoonotic Concerns
Bartonella spp can be transmitted to humans via a bite or scratch (cat, dog, or rabbit scratch disease).3,4,40,41
Research in cats has shown that claws contaminated with flea feces are the predominant source of infection.42
B henselae DNA has been PCR amplified from cat and dog saliva.43 Both cat and dog bites have been implicated in transmission to humans, and cat bites may be implicated in transmission to dogs; research into whether salivary transmission may occur from animals not infested by fleas is inconclusive.1,3
Needle stick transmission of B vinsonii subsp berkhoffii from a dog to a veterinarian has been reported.44
Veterinary workers are occupationally at risk of acquiring infection with Bartonella species.23,45
Listen to this podcast on Bartonella Species of Human Significance about the occupational hazards of Bartonella spp exposure and how to limit risks.
The author wishes to acknowledge the members of the North Carolina State University College of Veterinary Medicine Vector Borne Diseases Diagnostic Laboratory for generating the Bartonella spp serology data provided in the maps, as well as Brittany Thomas and Emily Kingston for data assimilation and map generation.
Dr. Breitschwerdt discloses that he is codeveloper of the Bartonella alpha–Proteobacteria growth medium enrichment blood culture platform, which is offered on a fee-for-service basis by the North Carolina State University Vector Borne Diseases Diagnostic Laboratory, which he co-directs.