Bone Marrow Core Biopsy
John W. Harvey, DVM, PhD, DACVP (Clinical Pathology), University of Florida

Overview
Bone marrow evaluation is indicated when certain peripheral blood abnormalities are detected. The most common indications are persistent neutropenia, unexplained thrombocytopenia, poorly regenerative anemia, or a combination thereof. Examples of proliferative abnormalities in which bone marrow examination may be indicated include persistent thrombocytosis or leukocytosis, abnormal morphologic characteristics of blood cells, or the unexplained presence of immature cells in blood (e.g., nucleated erythroid cells in the absence of polychromasia or neutrophilic left shift in the absence of inflammation).
Bone marrow is sometimes examined to stage neoplastic conditions (lymphomas and mast cell tumors), estimate the adequacy of body iron stores, and evaluate lytic bone lesions. Bone marrow evaluation can be useful to determine the cause of hyperproteinemia secondary to multiple myeloma, lymphoma, leishmaniasis, and systemic fungal diseases. It may also be examined for the presence of infectious organisms without coincident hyperproteinemia. Finally, bone marrow examination may reveal the underlying reason for hypercalcemia when present (lymphoid neoplasms, multiple myeloma, or metastasis of neoplasms to bone).
Procedure Pearl
Gathering both aspirate and core biopsies simultaneously is the optimum way to obtain information.
Core Biopsy Versus Aspiration
Aspiration biopsy of bone marrow is done more frequently than core biopsy in veterinary medicine because it is easier, faster, and less expensive and also because it more accurately identifies individual cell types, stages of cell development, and morphologic abnormalities of cells. Collection and preparation of bone marrow aspirate biopsy smears were described in the February 2004 issue (page 44) of NAVC Clinician's Brief.
Core biopsy sections provide a more accurate way to evaluate marrow cellularity and to examine for myelofibrosis, granulomatous diseases involving bone marrow, and metastatic neoplasia than do aspirate smears. Gathering both aspirate and core biopsies simultaneously is the optimum way to obtain information. Core biopsies are essential if there are repeated dry taps (i.e., failures to collect marrow particles by aspiration). Dry taps may result from technical error, but they can also occur when the marrow is packed with cells, as in cases of leukemia, and they usually occur when myelofibrosis is present. Dry taps or poor-quality samples are common when marrow aspirates are attempted on very young animals, even though the marrow is generally highly cellular.
There are few contraindications for bone marrow core biopsy. Postbiopsy hemorrhage is a potential but rare complication in patients with hemostatic diatheses. Hemorrhage that occurs after biopsy of an animal with monoclonal hyperglobulinemia is easily controlled by placing a suture in the skin incision and applying pressure over the biopsy site. Postbiopsy infection is also a potential complication but it is highly unlikely if aseptic technique is used.
Procedure Pearl
The ilium is generally too thin in cats and small dogs to collect a core sample parallel to its long axis, as is done in medium to large dogs. Two or three perpendicular punch biopsies passing completely through the most dorsal aspect of the wing of the ilium are substituted.
Biopsy Sites
Active marrow is present in the flat bones (pelvis, sternum, ribs, and vertebrae) and proximal ends of the humerus and femur in adults. The iliac crest may be used as a site for core marrow biopsies in dogs and cats (Figure A). In medium to large dogs, position the biopsy needle so that it enters the greatest prominence of the iliac crest parallel to the long axis of the wing of the ilium. The ilium is too thin to collect core biopsies in this manner in cats and small dogs. To collect core biopsies from the wing of the ilium in smaller animals, position the biopsy needle perpendicular to the wing of the ilium and obtain short cores by making two or three perpendicular punch biopsies completely through the most dorsal aspect of the wing of the ilium. If using this approach, remove the stylet when the needle touches bone, apply moderate pressure to the needle, and advance it completely through the wing of the ilium while rotating it in alternating clockwise-counterclockwise directions. The short cores that are obtained have cortical bone on both ends. Several cores are needed to obtain a sufficient sample for evaluation.
In contrast to aspirate biopsies, core biopsies are generally unsuccessful when attempted from the head of the proximal femur by way of the trochanteric fossa. The anterior side of the proximal end of the humerus is a popular site for core biopsies, especially in obese patients. The greater tubercle is palpated, and the needle is inserted into the flat area on the craniolateral surface of the proximal humerus distal to the tubercle (Figure B). Biopsies may be taken from other sites if specific lesions are identified using diagnostic imaging.
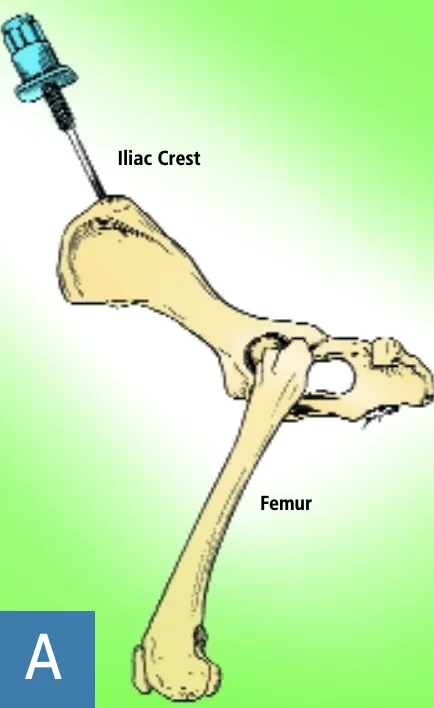
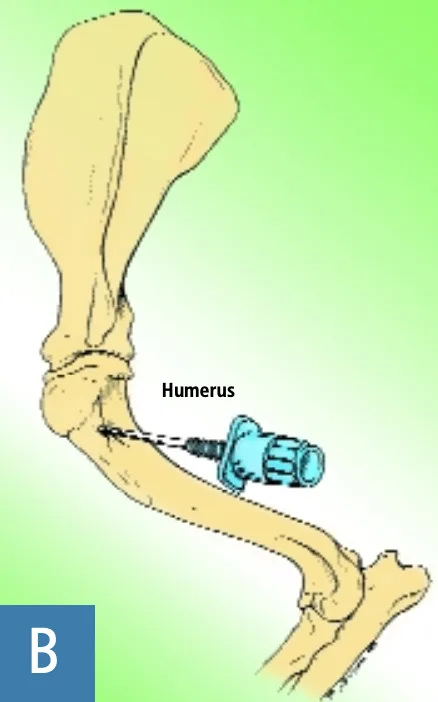
Figures A & B. Adapted/reprinted from Bone marrow biopsy and evaluation. Grindem CB. Vet Clin North Am Small Anim Pract 19:669-696, 1989, with permission from Elsevier.
If done at the same time, core and aspirate biopsies should be taken from distantly located sites (preferably different bones) to ensure that the biopsy does not disrupt the area from which the other biopsy is taken. Collecting biopsies from two separate sites should also increase the likelihood of identifying a metastatic tumor.
How to Perform Core Biopsy
What You Will Need
What you will need
Special needles—designed to cut a solid core of material are required. We use 11- to 13-gauge Jamshidi bone marrow biopsy needles that are 3 to 4 inches in length. An 11-gauge needle with stylet in place and the accompanying wire used to push the core biopsy from the needle are shown here.
Fixative—Formalin fixative is shown here. Other fixatives are sometimes preferred by pathologists; consult your surgical pathology service before collecting the sample to determine which to use.
Sample Submission

Photograph courtesy of Dr. Heather Wamsley
Submit the marrow core in fixative to a surgical pathology service. There, it will be decalcified, embedded, sectioned, stained with hematoxylin and eosin and possibly other stains, and examined microscopically by a pathologist. Unstained aspirate smears, core roll preparations, and other exfoliative cytology preparations should not be mailed in the same package with formalin-fixed tissue because formalin vapors interfere with the staining quality of cells in the cytologic preparations.
Step 1
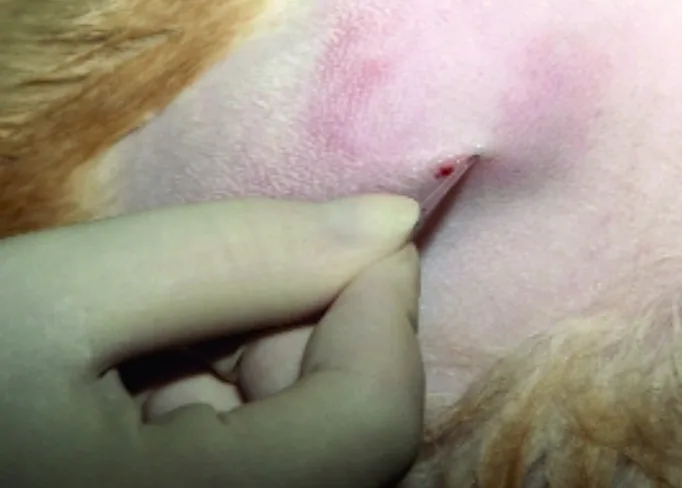
Most animals are tranquilized before bone marrow biopsy. Prepare the biopsy sites by clipping the hair and scrubbing the skin with antiseptic soap. In this case the flat area on the craniolateral surface of the proximal humerus distal to the greater tubercle is shown.

Step 2
Inject a local anesthetic under the skin and down to the periosteum overlying the biopsy site. Make a small skin incision with a scalpel blade to facilitate passing the needle through the skin. Sterile needles, syringes, and gloves are always used, but the core biopsy site need not be draped. Light general anesthesia may be necessary in some cats. If general anesthesia is required for other procedures, bone marrow core biopsy may be scheduled at the same time to minimize the stress on the animal.
Step 3
With the stylet locked in place, apply moderate pressure to the needle while rotating it in an alternating, clockwise-counterclockwise direction.

Step 4, 5
Once the needle is firmly embedded into the bone, remove the stylet (and needle cap, if present) and advance the needle using the same clockwise-counterclockwise motion. If possible, advance the needle 1 inch or more to collect a sufficient sample for evaluation. Once the needle has been advanced to its maximal depth, make several 360-degree twists and withdraw.


Step 6
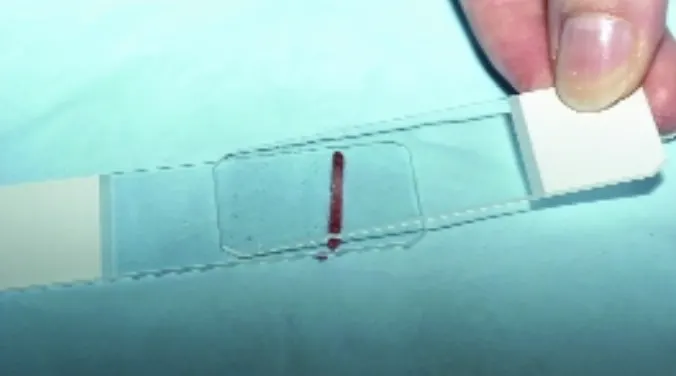
Push the core within the needle out onto a glass slide using the wire that accompanies the needle. Place the wire in the tip of the needle and force the core out of the handle end. Because the tip of the needle is tapered, pushing the core out through the tip would add crush artifacts to the core.

Step 7, 8
If attempts to aspirate bone marrow result in dry taps or poor-quality smears, the core biopsy may be gently rolled across a glass slide using a second glass slide. The resulting roll preparation is then stained with a routine blood stain, such as Wright-Giemsa. These roll preparations are generally of lower quality than aspirate smears. In particular, the number of megakaryocytes and amount of stainable iron present are generally underrepresented. After making one or more roll preparations, place the core in fixative. Because fixatives other than formalin are sometimes preferred by pathologists, consult your surgical pathology service before collecting the sample to determine which to use.