Blastomycosis in a Dog

Sadie, a 9-year-old spayed German shepherd, was presented for evaluation of a lower right forelimb skin lesion of a few weeks’ duration.
History
The owner did not recall any injury and reported the lesion had grown slowly; the dog had just started licking it. No other problems were reported, but the owner mentioned that Sadie had been slowing down recently—something she attributed to the dog's age.
Examination
The lesion was ulcerated with mild mucopurulent discharge but did not appear to extend into deeper tissue; there was no associated cellulitis.
The dog was bright, alert, and responsive. Sadie had a body condition score of 4/9, and her body weight had decreased from 34 kg to 31 kg since her last visit (approximately 18 months earlier). Lameness was not evident at a walk, and apart from the area with the skin lesion, she did not resent palpation of the leg. The lesion was approximately 1 × 2 cm, extending proximally and laterally from the nail beds of digits IV and V. The lesion was ulcerated with mild mucopurulent discharge but did not appear to extend into deeper tissue; there was no associated cellulitis. Vital parameters were normal, but moderately harsh lung sounds were detected bilaterally over the entire lung fields. Physical examination was otherwise unremarkable.
Diagnostic Testing & Treatment
A swab and impression smear of the lesion were collected for cytologic analysis. The owner declined further testing to evaluate weight loss and potential respiratory disease. After the lesion was cleaned and debrided with Sadie under sedation, a bandage was applied and Sadie discharged.
Cytology results were suggestive of blastomycosis based on the presence of abundant budding yeasts with a broad base (Figure 1). On further consultation, the owner revealed that Sadie regularly accompanies her on camping trips to an area near Georgian Bay, Ontario, where blastomycosis is endemic.
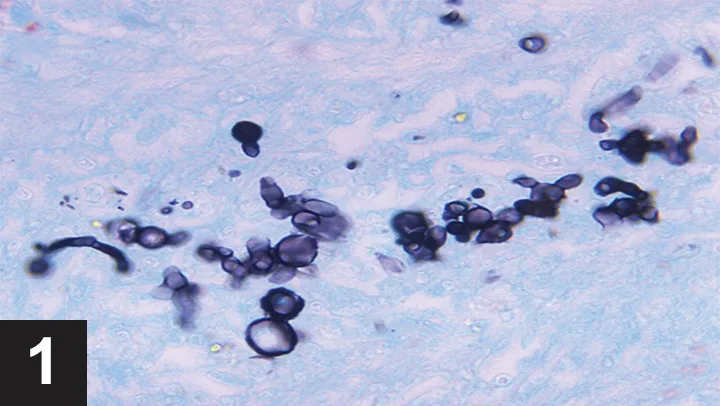
Blastomyces dermatitidis from a liver aspirate in a dog with blastomycosis. Note the typical budding yeasts. Image courtesy of Centers for Disease Control and Prevention—National Center for Zoonotic, Vector-Borne, and Enteric Diseases; Division of Foodborne, Bacterial and Mycotic Disease
The owner consented to further testing, and a radiographic pattern consistent with pulmonary blastomycosis was identified on thoracic radiographs (Figure 2). Ocular examination was unremarkable. Mild leukocytosis and monocytosis were evident on CBC, while the serum chemistry panel was unremarkable. A urine sample was submitted for Blastomyces dermatitidis enzyme immunoassay (EIA) for additional confirmation, and treatment with itraconazole was started.

Thoracic radiograph of a dog with blastomycosis. Note the nodular interstitial pattern with patchy alveolar infiltrates. Image courtesy Dr. Shawn MacKenzie
Both the veterinary technician, who assisted with wound care, and the owner expressed concern about exposure to this fungal pathogen.
Ask Yourself
Blastomyces dermatitidis is a dimorphic yeast and therefore occurs in 2 forms, as a yeast and a mold (mycelial form; Table). The mold (mycelial) form is the infectious phase that lives in the environment at ambient temperature, while the yeast phase is present in infected tissue at body temperature.
Table: Yeast & Mold Forms of Blastomyces dermatitidis
* No externally validated assays are available.
** Culture, which can be exceedingly difficult, should only be performed by experienced laboratories using biosafety level 3 containment. In-house fungal culture should never be attempted in animals that might have blastomycosis.
Infection typically occurs from inhalation of the mold spores, which can be found in the environment in endemic regions. These spores convert to yeast form in the lungs, propagate, and disseminate hematogenously, potentially causing pulmonary or extrapulmonary disease, often involving the skin, eyes, and lymph nodes.
The yeast form of B dermatitidis is not transmissible to other animals (including humans) under normal circumstances, as it must be directly inoculated into tissue to cause disease. Risks posed by the yeast form are predominantly associated with bites, needlestick injuries, or other sharps injuries. Transmission of B dermatitidis to a veterinarian has occurred as a result of a needlestick injury following a fine-needle aspiration of an infected site.1 While infection via this route has been rarely reported, it should be considered because of the typically lax sharps-handling practices often seen in veterinary hospitals and the relatively high incidence of needlestick injuries.2,3 Particular care should be taken with sharps handling in any animal with suspected blastomycosis, especially after fine-needle aspiration of a lesion.
A bite from an infected animal is another potential route of transmission, as this can inoculate the yeast form into tissue.4,5
Another potential (but unproven) concern is reversion of the yeast form to the infectious mold form on bandage materials or exudates deposited in the environment. Yeast–to–mycelial conversion can occur within 3 to 4 days at room temperature, suggesting there could be a risk associated with contaminated surfaces or materials. This route of transmission, however, has not been documented.
Basic infection-control practices (eg, prompt disposal of bandages, regular bandage changing, proper waste disposal, routine cleaning and disinfection) should greatly minimize any theoretical risk for transmission of B dermatitidis.
The Take-Home
There is limited risk for transmission of Blastomyces dermatitidis from infected patients.
Extra care should be taken to reduce the risk of sharps injury, especially after fine-needle aspiration of an infected site.
Contaminated bandage materials should be promptly disposed of as biohazardous waste.
Although bite-associated blastomycosis is very rare, owners should be counseled about the potential risk and the need to consult a physician if the dog bites anyone during treatment.
EIA = enzyme immunoassay, PCR = polymerase chain reaction
J. SCOTT WEESE, DVM, DVSc, DACVIM, is veterinary internist and microbiologist, chief of infection control at University of Guelph Ontario Veterinary College Health Sciences Centre, and Canada research chair in zoonotic diseases. Dr. Weese’s research foci are infectious and zoonotic diseases (particularly of companion animals), infection control, staphylococcal infections, Clostridium difficile infection, and antimicrobial therapy.