How to Clean the Canine Ear

Otitis externa is common in small animal medicine, representing 10% to 20% of cases seen. The type of ear cleaning described here is considered "major ear cleaning" and is performed under heavy sedation or general anesthesia.
Excess debris must be removed for appropriate evaluation of the ear canal and tympanic membrane. Removing excess wax and debris increases treatment efficacy through better penetration of topical medications. Proper ear cleaning removes bacterial by-products, degenerating cells, and free fatty acids that contribute to inflammation. Also, pus and inflammatory debris inactivate some antimicrobial agents.
Pro Pearl: Samples for culture and sensitivity should be obtained before flushing the ear canal.
Ear Cleaning Instruments and TechniquesVarious techniques have been described for ear cleaning, varying from the bulb syringe to sophisticated flushing systems. I prefer to flush with bulb syringes and a feeding tube-syringe technique combined (see What You'll Need). Increasing availability of fiberoptic otoscopes have made otic examination and cleaning much easier due to improved visualization. However, effective cleaning can be done without such equipment.
Pro Pearl: Saline is preferred for flushing because the condition of the tympanic membrane is often unknown.
Ear Canal AnatomyKnowledge of ear canal anatomy is helpful during otic examination and cleaning. Cleaning techniques generally focus on the external ear canal, which comprises vertical and horizontal canals.
The canal is generally 2 cm in length and varies from 5 to 10 mm in diameter, depending on breed and size. Lining of the external ear canal contains sebaceous and ceruminous (apocrine) glands. Hair follicles occur throughout the canal; follicle density varies among breeds. Sebum found in the ear canal is sebaceous and ceruminous gland secretions and epithelial cells combined.
The tympanic membrane (TM) separates external and middle ear canals. The TM is thin and opaque, comprising the pars tensa (tightly stretched opaque section) and pars flaccida (dorsal component covering part of the malleus). The middle ear comprises the tympanic cavity and bullae. This cavity can often be viewed if the TM is completely ruptured.
Epithelial migration plays a role in "self-cleaning" of the ears. Migration and production of sebum cause normal accumulation of waxy brown debris on the ventral aspect of the ear canal just distal to the TM.
Pro Pearl: Sedation or general anesthesia is required for proper cleaning and visualization.
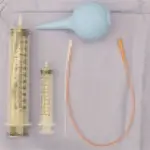
What You'll Need• Alligator forceps• Ear curettes• Sterile saline (room temperature or lukewarm)• 6-ml and 12- or 20-ml syringes• Red rubber feeding tubes (5 French, cut [Abbott Labs] to various lengths)• Open-ended Tom Cat catheter (3 French [Kendall])• Disposable rubber ear bulb syringes [Jorgensen Laboratories]• Ceruminolytic agents (Clear-X [DVM Pharmaceuticals] or Cerumene [Evsco Pharmaceuticals])• Hand-held otoscope with surgical head and cones [Welch Allyn]• Fiberoptic otoscope [Storz, Med Rx]
Step-by-Step Instructions
Obtain samples for culture and sensitivity from the external ear canal before flushing. If otitis media is suspected, perform myringotomy with an open-ended Tom Cat catheter and a sterile 6-ml syringe filled with nonbacteriostatic sterile saline. Puncture the TM, and flush and aspirate the contents of the middle ear. Myringotomy should be done with great care to avoid damaging middle ear structures. This is best accomplished by puncturing the TM between 5 and 7 o'clock. If the TM is intact, you can feel the catheter tip break through the membrane. Then flush and aspirate the contents of the middle ear. This sample should be submitted for aerobic culture and sensitivity. Two sets of cultures may be needed - one from the canal and one from the tympanic bullae.

Otitis with severe purulent and ceruminous discharge
Heavily sedate or anesthetize the patient since head shaking or movement makes evaluation difficult. Sedation with acepromazine alone is generally inadequate. General anesthesia is recommended if the patient is anxious or ears are painful. When deep ear cleaning and myringotomy are necessary, administer deeper anesthesia to prevent movement and pain. Make sure the endotracheal cuff is appropriately inflated to prevent flushed matter from entering the nasopharynx.
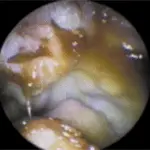
Swollen, purulent ear canal before cleaning
Several techniques can be used to flush and clean ears. I prefer to start by using the bulb syringe technique.
**
Bulb syringe technique**1. Flush the canal gently with sterile saline. I always use saline for flushing because the condition of the TM is often unknown. Other flushing agents, such as chlorhexidine or diluted povidone-iodine, can be contraindicated if the TM is not intact.2. Massage the ear canal externally for 1 to 2 minutes, and suction the fluid with a bulb syringe. Make sure the syringe does not fit too tightly within the ear canal, which creates a vacuum and may rupture a possibly diseased TM.3.Reexamine the canal; evaluate for patency and the condition of the TM. If a large amount of ceruminous debris is present in the ear canals, use a ceruminolytic agent (e.g., Clear-X and Cerumene). Such agents emulsify waxes and lipids, facilitating removal. These agents require a contact time of 5 to 15 minutes for maximum effectiveness.4. Since ceruminolytic agents can be irritating, flush the ear canal thoroughly with saline. Generally 250 to 350 ml/ear is used.
Pro Pearl: Make sure the syringe does not fit too tightly within the ear canal, which creates a vacuum and may rupture a possibly diseased TM.
Stronger agents may be contraindicated with a ruptured tympanum (often difficult to determine before cleaning and examination). This flushing technique is effective for cleaning external ear canals only, not if a false middle ear is present or for flushing the middle ear (tympanic bulla).
A false middle ear is created when chronic pressure from contents within the horizontal canal causes the TM to stretch into the tympanic cavity. This is difficult to assess with a hand-held otoscope.
Red rubber feeding tubes and syringes (12 or 20 ml) are effective for canal flushing when these conditions exist.
Red Rubber Feeding Tube and Saline
This technique can be performed through the surgical head of a hand-held otoscope or through the flushing port of a fiberoptic video otoscope. These tools enable better visualization of where the tip is located (and where it needs to be directed).
Flushing with red rubber feeding tube and saline as seen through otoscope
Pro Pearl: A ceruminolytic agent may be necessary if a large amount of ceruminous debris is present in the ear canal.

1. Cut the end off the feeding tube to create an opening. Pass the catheter through the surgical head of the otoscope. Attach other end of tube to the syringe filled with sterile saline.
2. Direct the tip where desired and infuse saline into the canal. A gentle back-and-forth motion helps dislodge debris.3. Use the syringe and catheter to aspirate fluid and debris. Depending on how much debris is present, flushing and aspirating may need to be repeated using 250 ml total of saline. This technique is preferred if the eardrum is ruptured and is the most effective way to dry the ear canal.
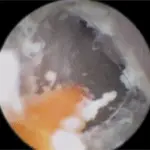
Canal after cleaning, with evidence of moderate irritation from flushing
Curette and ForcepsThe ear canal and TM can now be re-evaluated. If debris remains, an ear curette or alligator forceps may be used. These instruments are especially effective at removing small wax plugs, foreign bodies, or keratin plugs. Gently pull the curette along the lining of the canal to dislodge debris and pull it to the opening of the ear canal. These instruments can also be passed through the head of the otoscope for maximum visualization. Alligator forceps can be used to grasp foreign bodies or firmer debris. I have not had significant success with suction devices. The main disadvantages include no effective way to flush the canals, difficulty in accessing the middle ear (tympanic bulla), and difficulty in cleaning the suction tubing and equipment.
Pro Pearl: Alligator forceps can be used to grasp foreign bodies or firmer debris.
Follow-up MedsAfter ear cleaning, I generally administer short-term antiinflammatory corticosteroid medications to help reduce pain and inflammation (single injection of 0.1-0.2 mg/kg dexamethasone IV or SC). Neurologic symptoms (deafness, vestibular syndrome) are rare after ear flushing but can occur even if ototoxic medications have not been used. Symptoms may resolve when inflammation has lessened or may be permanent. Complications are more common in cats than dogs.
Pro Pearl: Myringotomy is best performed at the 5- to 7-o'clock location.