Weakness & Exercise Intolerance in a Dog

A 10-year-old, castrated Labrador retriever was presented for excessive salivation.
HistoryAccording to the owners, the dog’s onset of hypersalivation was recent and his regular veterinarian had prescribed maropitant citrate at 60 mg PO q24h for apparent nausea and topical mometasone furoate (small amount in ear q24h for 7 days) for confirmed otitis externa of the left ear. Follow-up 1 week later showed persistent salivation and otitis externa, along with apparent pain on neck palpation and weight-bearing lameness of the right thoracic and left pelvic limbs. The dog was referred for neurologic evaluation.
Neurologic ReferralThe dog was alert and responsive with normal hydration status. Physical and orthopedic examinations were unremarkable except for a finding of mild weight-bearing lameness of the right thoracic and left pelvic limbs. The previously reported hypersalivation and apparent cervical pain were not evident. During continuous walking, the dog’s gait became progressively short-strided in all limbs, until it collapsed and was unable to stand. The dog recovered after resting for a few minutes and was able to resume a gait similar to that seen before the exercise-induced collapse. Additional abnormalities were not detected on neurologic examination. Results of CBC, serum biochemical profile, and total T4 were unremarkable.
Ask Yourself:1. If the patient is neurologically abnormal, what is the neuroanatomic localization of signs?2. What is the primary differential?3. What is the MDB that should be obtained for this condition?4. What screening test could increase the index of suspicion for the most likely neurologic cause of exercise-induced collapse, and how does it work?5. Which laboratory test is most likely to confirm the diagnosis?
Diagnosis: Generalized neuromuscular disorder
Preliminary DiagnosisInitial gait analysis suggested that the lameness resulted from an orthopedic condition, as the initial neurologic examination was normal (see Collapse: Neurologic or Not?). However, the patient developed a progressively short-strided gait in all 4 limbs while walking around the hospital. Short-strided gait can be caused by disease affecting the spinal intumescence of the affected limb(s), orthopedic conditions, or peripheral neuromuscular disease. Because all limbs were affected, both cervical and lumbar intumescence would have to be affected. This was unlikely because ataxia or apparent spinal pain was not present, and the postural reactions and segmental reflexes remained normal even as the patient became progressively weaker.
Related Article: The Case: Coughing, Gagging, & Ataxia in a Young Terrier Mix
Collapse: Neurologic or Not?Possible differentials for exercise-induced collapse in dogs include:
Nonneurologic
Bone/joint disorders (eg, polyarthritis)
Cardiovascular disorders (eg, subvalvular aortic stenosis)
Respiratory disorders (eg, laryngeal paralysis, pulmonary parenchyma or pleural space abnormalities)
Anemia
Hypoglycemia
Hypoadrenocorticism
Hypothyroidism
Neurologic
Generalized neuromuscular disorders (eg, MG, polymyositis, metabolic myopathies, acquired peripheral polyneuropathies)
Acquired spinal cord disease (eg, chronic intervertebral disk disease)
Orthopedic disease was considered less likely, as no orthopedic abnormalities (eg, joint pain or effusion) were detected. As a result, generalized neuromuscular disease was considered the likely localization. Myasthenia gravis (MG) was the primarydifferential because it is the disease most frequently identified in dogs with exercise-induced collapse, laryngeal/pharyngeal weakness (eg, excessive salivation, gagging/retching), and generalized weakness. Other differentials included myopathies (eg, polymyositis, degenerative myopathies), polyneuropathies, and orthopedic diseases (eg, polyarthritis).

DiagnosticsThe results of CBC and serum biochemistry profile were within normal limits. An edrophonium challenge (Tensilon test) was scheduled and the patient treated with atropine at 0.03 mg/kg IV 15 minutes before the test to reduce risk for cholinergic crisis. The dog was exercised to fatigue and then given edrophonium chloride at 0.15 mg/kg IV. Within 1 minute there was dramatic improvement in strength that lasted 2 to 3 minutes; this was considered a positive result that greatly increased the index of suspicion for acquired MG.
Related Article: Megaesophagus

Thoracic radiography and abdominal ultrasonography were performed to screen for an inciting cause of MG. Thoracic radiographs (Figure 1) showed a well-circumscribed, spherical-to-ovoid cranial mediastinal mass and moderate megaesophagus. Thymoma was considered the most likely cause. There was no evidence of aspiration pneumonia. Abdominal ultrasonography was unremarkable.
Figure 1. Lateral (A) and ventrodorsal (B) thoracic radiographs showing a round, circumscribed mass in the cranial thorax and moderate megaesophagus.
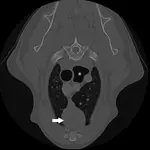
The following day, thoracic CT was performed to better evaluate the mass, determine the size of regional lymph nodes, and look for evidence of pulmonary metastasis. A well circumscribed, partially cystic mass was identified in the cranial mediastinum (Figure 2). There was no evidence of thoracic lymphadenopathy or pulmonary metastases. An ultrasound-guided, fine-needle aspirate of the mass was obtained; cytologic diagnosis was consistent with probable lymphocyte-predominant thymoma with mononuclear cell inflammation and hemorrhage.
Figure 2. Thoracic CT showing a circumscribed, cystic, round mass in the cranial mediastinum (arrow). Dilation of the gas-filled esophagus is also visible (*).
Serum was submitted for AChR antibody (AChR Ab) titer.
TreatmentThe patient was discharged on pyridostigmine at 1 mg/kg PO q12h and elevated feedings were initiated pending the AChR Ab titer result, which came back positive (6.73 nmol/L; normal, <0.6 nmol/L), confirming the diagnosis of acquired MG. In the first week after discharge, there was marked improvement, with the dog no longer showing evidence of lameness, weakness, or exercise intolerance.
After 1 week, a median sternotomy was performed. A peach-sized, encapsulated mass (Figure 3) in the cranial mediastinum was easily removed and confirmed as thymoma on histopathology. The patient recovered uneventfully and was discharged on continuing pyridostigmine therapy.
Figure 3. Intraoperative image of the mass, which was confirmed as thymoma on histopathology.
At the recheck neurologic examination 1 month later, the dog showed no evidence of exercise intolerance. Some mild hypersalivation persisted but had improved significantly. AChR Ab titer at that time was significantly lower (0.96 nmol/L), suggesting that thymoma was the cause of acquired MG because no immunosuppressive medications had been administered. The pyridostigmine dose was lowered by 25%.
OutcomeAt 2 months, the AChR Ab titer was negative (0.08 nmol/L). The pyridostigmine dose was lowered by 25% q1wk over the course of 1 month and then discontinued. Repeat AChR Ab titers at 3, 6, and 9 months were all negative, and the patient remained clinically normal.
Acknowledgments: The author extends gratitude to Lisa Corti, DVM, DACVS, CCRP, for the successful surgical outcome and for providing intraoperative photography, as well as to Jennifer Brisson, DVM, DACVR, and Tonya Tromblee, DVM, MS, DACVR, for assistance with diagnostic imaging.
Did You Answer?
1. The neuroanatomic localization of signs was likely generalized neuromuscular disease. Many dogs with significant generalized weakness have postural reaction deficits, but dogs with MG and other neuromuscular diseases sometimes have normal postural reactions if rested and/or only mildly weak.1 The absence of abnormalities on orthopedic examination suggested it was not an orthopedic condition. If the weakness had been caused by CNS disease, the dog would probably have been ataxic and/or had postural reaction deficits or changes in segmental spinal/withdrawal reflexes. Other diseases that can mimic neuromuscular disease and cause exercise intolerance include cardiovascular, endocrine or metabolic (eg, hypothyroidism, hypoadrenocorticism), and upper airway disease.
2. Acquired MG was the primary differential.
3. The MDB for acquired MG includes CBC, serum biochemistry profile, urinalysis, thyroid hormone profiles in older patients, thoracic radiography, and abdominal ultrasonography to rule out other causes of generalized weakness and search for diseases frequently associated with acquired MG (eg, neoplasia, hypothyroidism, hypoadrenocorticism). Thoracic radiographs should be evaluated for megaesophagus, aspiration pneumonia, and thymoma.
4. Edrophonium challenge (Tensilon test) can increase the index of suspicion. Acquired MG is caused by auto- immune destruction of nicotinic AChR at the neuromuscular junction of skeletal muscle. Edrophonium is a rapid-onset, short-acting anticholinesterase inhibitor. By inhibiting the enzyme that breaks down ACh at the neuromuscular junction, ACh remains in the neuro- muscular junctions longer, allowing it to bind to available AChR. This, in turn, leads to improved strength. The Tensilon test can be used as quick in-hospital screening for MG but lacks sensitivity and specificity; there is a high rate of false-negative results (~30%). If edrophonium is not readily available, another easy screening tool is quick, repetitive palpebral (blink) or patellar reflex testing. A recognizable decrease of these reflexes with repetitive testing suggests MG.
5. The most easily available and reliable test for diagnosing acquired MG in dogs is detection of antibodies directed against the AChR. Approximately 2% of myasthenic patients are seronegative. False-positive results are rare. Other tests that confirm the diagnosis of acquired MG include repetitive nerve stimulation, single-fiber electromyography, or histologic examination of the neuromuscular junction after whole-muscle biopsy (eg, of the external intercostal, peroneus longus).
MARK TROXEL, DVM, DACVIM (Neurology), is neurologist and neurosurgeon at Massachusetts Veterinary Referral Hospital in Woburn, Massachusetts. His clinical interests include canine and feline brain tumors, vestibular dysfunction, and neurosurgery, topics on which he frequently lectures at local, regional, and national meetings. Following a rotating internship in small animal medicine, surgery, and critical care at VCS South Shore Animal Hospital in South Weymouth, Massachusetts, and internship in internal medicine at Garden State Veterinary Specialists in Tinton Falls, New Jersey, Dr. Troxel completed a residency in medical neurology and neurosurgery at University of Pennsylvania. He earned his DVM from Iowa State University.
WEAKNESS & EXERCISE INTOLERANCE IN A DOG • Mark Troxel
Reference
Veterinary Neuroanatomy and Clinical Neurology, 3rd ed. DeLahunta A, Glass EN—St. Louis: Saunders Elsevier, 2009.
Suggested Reading
Myasthenia gravis and disorders of neuromuscular transmission. Shelton GD. Vet Clin North Am Small Anim Pract 32:189-206, 2002.Myasthenia gravis in dogs with an emphasis on treatment and critical care management. Khorzad R, Whelan M, Sisson A, Shelton GD. JVECC 21:193-208, 2011.Results of excision of thymoma in cats and dogs: 20 cases (1984-2005). Zitz JC, Birchard SJ, Couto GC, et al. JAVMA 232:1186-1192, 2008.