Pseudomonas Otitis Infection in Cats and Dogs
Susan Paterson, VetMB, MA, DVD, DECVD, FRCVS, Virtual Vet Derms, Kendal, United Kingdom

Profile
Definition
Pseudomonas otitis is an infection of the ear (Figure 1, see above), most commonly with P aeruginosa, a motile gram-negative bacillus ubiquitous in the environment but uncommon in the canine or feline ear.
P aeruginosa grows within moist environments (eg, soil, vegetation, feces).
This predisposition makes infectious otitis caused by P aeruginosa more common in tropical climates.
Signalment
Breed Predilection
Pseudomonas otitis occurs in dogs and cats.
Dogs with hairy, narrow canals and pendulous pinnae (eg, cocker spaniel) are predisposed to P aeruginosa infection.
No breed predilection is recognized in cats.
Age
Pseudomonas spp infections occur at any age.
In younger patients, infection is commonly associated with allergy or ectoparasites.
Young cats may have nasopharyngeal polyps as underlying triggers.
In older patients, immunosuppression (from systemic or endocrine disease) or neoplasms of the external ear canal can increase risk.
Causes
Pseudomonas spp rarely infect “normal” tissue, so causes should be identified.
Two studies in dogs1,2 have suggested that primary triggers for Pseudomonas spp are not always evident, but infection can be associated with foreign bodies, grooming, and bathing.
Risk Factors
At-risk factors include those that disrupt the normal environment within the ear canal and allow bacterial invasion:
Disruption to the physical barrier.
Changes affecting ventilation of the ear canal (eg, humidity, cerumen composition, temperature).
In dogs, conformation of the ear canal and pinna (eg, spaniels).
In cats, changes to otic environment; infection with nasopharyngeal polyps.
Immune system dysfunction also is a common factor.
Long-term use of weak antiseptics, to which Pseudomonas spp are inherently resistant, or chronic antibiotic use (systemic/topical) without addressing underlying disease.
Endocrine disease (eg, hypothyroidism, hyperadrenocorticism).
Systemic disease (eg, renal, hepatic, pancreatic disease).
Cats with FeLV or FIV.
Pathophysiology
In acute otitis, dermal edema can lead to altered barrier function and changes in cerumen composition.
In the canal, changes lead to increased gram-positive bacteria.
As the lumen narrows, ventilation is reduced, environment becomes more anaerobic, and humidity and temperature increase.
These events lead to bacterial population of predominantly gram-negative flora, especially Pseudomonas spp.
P aeruginosa has mechanisms for evading the host’s immune response:
Toxins and proteases (eg, exotoxin A, lecithinase).
Glycocalyx “slime” helps protect P aeruginosa against influences from immune system and topical medication.
Signs
Otic infection with Pseudomonas spp is usually a unilateral disease with acute onset.
Animals typically present with head shaking or ear scratching.
Infected ear pinna is commonly inflamed and often ulcerated.
Otic discharge, which can extend onto the concave aspect of the ear pinna, is usually mucoid, malodorous, and yellow/green.

History
The first sign owners usually notice is malodorous discharge.
Owners may also report signs of neurologic damage (eg, Horner syndrome, facial nerve paralysis):
Motor nerve damage appears as facial asymmetry.
Parasympathetic nerve damage may appear as keratoconjunctivitis sicca.
Animals may have problems chewing hard food, barking, or carrying objects.
With otitis interna, owners may report hearing loss, head tilt, or nystagmus.
Physical Examination
Patients usually resent ear examination.
Their ears are painful rather than pruritic.
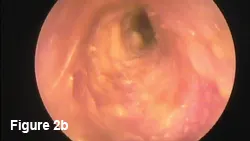
The ear canal is swollen, ulcerated (Figure 2, Video otoscope images of an ulcerated, erythematous, inflamed ear in a dog with Pseudomonas infection.), and uncomfortable with malodorous, often hemorrhagic yellow/green mucopurulent discharge.
The tympanum may or may not be intact.
It can remain intact while the middle ear is infected but will appear abnormal (eg, bulging, hemorrhagic, dark [brown/gray] with visible exudate behind it).
When infection involves the middle ear, animals may show signs of otitis media or interna.
Otitis media (with/without tympanic rupture) is reported in ~83% of chronic otitis externa cases.7
Pain Index
The density of nerve endings increases with ear depth.
Although inflammation and ulceration commonly extend from pinna into middle ear, involvement of horizontal canal and middle ear contributes to severe pain.
This makes adjunct analgesia important.
Diagnosis
Definitive Diagnosis
Infected pinnae are typically erythematous, ulcerated, and covered in thick yellow/green mucoid discharge.
Otoscopic examination (may require sedation/anesthesia) reveals further inflammation and ulceration of the canal, which is often swollen and partially occluded.
Discharge in the canal is similar to that on the pinna but often is hemorrhagic.
Differential Diagnosis
Underlying causes can vary and trigger factors should be thoroughly investigated.
Factors may include concurrent systemic disease, inappropriate therapy, or changes to the ear canal’s microclimate.
Laboratory Findings
Cytology
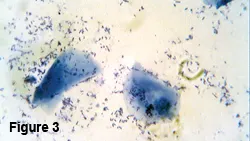
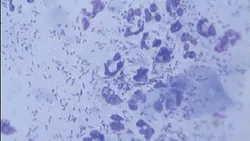
Samples of otic exudates should be stained with Gram or modified Wright’s-Giemsa stain.
P aeruginosa appears as rod-shaped organisms, typically accompanied by degenerate neutrophils (Figure 3, Cytology of a sample obtained from the external ear canal showing Pseudomonas spp infection with numerous rod-shaped organisms (400¥ original magnification).
Rod bacteria on cytology samples of otic exudates should undergo culture and antibiotic sensitivity testing.
Cultures
Samples for cytology should be obtained from the junction of vertical and horizontal canals.
In cases of suspected otitis media, samples from the middle ear are needed.
Samples of bacteria can be obtained with guarded technique by passing a sterile swab or syringe attached to a 4-5 French gauge catheter (through which 0.5 mL of sterile saline can be instilled and suctioned) down a clean, handheld otoscope cone.
Myringotomy should be performed if the tympanic membrane is intact but abnormal.
Myringotomy involves a catheter penetrating the pars tensa in the caudoventral quadrant of the tympanum catheter, accessing the middle ear.
When the tympanum is intact, it is important to obtain 2 samples (1 each from horizontal canal and middle ear), as bacterial isolate type and antibiotic sensitivity may differ.
Imaging
Imaging is useful when otitis media is present.
Open-mouth and lateral oblique radiographic views are most informative.
However, radiography is a poor modality for viewing mild bony changes.
CT and MRI are superior for assessing changes within the tympanic bulla.
If the tympanic bulla has excessive bony change or contains large amounts of granulation tissue, prognosis for resolution by medical therapy alone is poor.
Treatment
Inpatient or Outpatient
All Pseudomonas otitis cases benefit from thorough cleansing.
When cleansing the canal and middle ear, pain is best minimized with the patient under general anesthetic in a hospital environment.
After cleansing, treatment can be on outpatient basis.
Medical
Otitis externa is treated using topical flushes and antibiotics.
Benefits and use of systemic antibiotics for otitis externa (without otitis media) are controversial.
In cases of otitis media, licensed topical medications may not be appropriate because of risks for ototoxicity; off-license topical therapy may be indicated (with client consent).
Surgical
When examination and imaging demonstrate irreversible ear damage, surgical intervention is indicated.
When both canal and middle ear are involved, total ear canal ablation and bulla osteotomy may be necessary.
When damage is confined to the middle ear, a ventral bulla osteotomy may be more appropriate.
Medications
Glucocorticoids
Systemic and topical glucocorticoids reduce formation of exudate and swelling (and pain associated with inflammation).
An antiinflammatory dose of dexamethasone is invaluable at initial flush.
Follow-up with topical glucocorticoids incorporated into medication (eg, dexamethasone, betamethasone, mometasone) and/or antiinflammatory doses of systemic prednisolone.
Cleaners & Flushes
Ear cleaners and flushes (see Flush Solutions & Antibiotic Options) can be used to remove infected debris and inflammatory mediators.
They break up mucus produced by mucoperiosteum of inflamed middle ear and Pseudomonas spp.
Adequate flushing provides pain relief and allows penetration of topical antibiotics.
Acetic acid at 2% solution is lethal to Pseudomonas spp within a minute of contact.3,4
Tris-EDTA is also a useful flush.
May be prepared as solution or concurrently with other topicals (eg, chlorhexidine).
Tris-EDTA increases permeability of Pseudomonas spp cell membranes by binding calcium and magnesium ions.5
Presoaking the ear canal with tris-EDTA helps potentiate aminoglycoside and fluoroquinolone antibiotics.5,6
Flush Solutions & Antibiotic Options
Flush Solutions
Acetic acid (Malacetic, dechra-us.com)
Tris-EDTA (TrizEDTA, dechra-us.com)
Topical Antibiotics—First Line
Enrofloxacin–silver sulfadiazine (Baytril Otic, bayerdvm.com)
Gentamicin (Easotic, virbacvet.com; Otomax and Mometamax, merck-animal-health-usa.com)
Marbofloxacin (Aurizon, vetoquinolusa.com)
Polymyxin (Surolan, vetoquinolusa.com)
Topical Antibiotics—Second Line
Amikacin injectable (dilute 250 mg/mL–50 mg/mL) 4–8 drops of 50 mg/mL q12h
Ticarcillin or ticarcillin and clavulanic acid (Timentin, us.gsk.com)
Silver sulfadiazine (Silvadene cream [diluted with water] or powder for 1% solution)
Ceftazidime
Topical Antibiotics—Off-License Use
Dilute topical antibiotics in 12 mL tris-EDTA; instill 0.5 mL into ear q12h after flushing
Gentamicin 1 mL (40 mg/mL) (roche.com)
Enrofloxacin 4 mL (2% solution) (bayerdvm.com)
Marbofloxacin 4 mL (1% solution) (vetoquinolusa.com)
Antibiotics
Topical antibiotics, such as polymyxin, gentamicin, and fluoroquinolones (ie, enrofloxacin, marbofloxacin), are useful.
Ear drops with these agents are only appropriate with intact tympanum.
Aqueous solutions of gentamicin, marbofloxacin, and enrofloxacin are safe for ruptured ear drums.
Potential second-line drugs include amikacin, tobramycin, ceftazidime, silver sulfadiazine, and ticarcillin as off-licensed preparations.7-9
Systemic antibiotics should be used when otitis media is present1; however, levels of antibiotics within the bulla will be far lower than when topically instilled.
Systemic medication may be the only possible therapy when the canal is swollen and hyperplastic, the owner cannot treat topically, or topical medication incited an adverse reaction.
Systemic therapy includes oral fluoroquinolones and injectable amikacin, based on results of culture and sensitivity testing.
Pain Management
Opioids (eg, buprenorphine, butorphanol, tramadol) provide pain relief.
NSAIDs are generally less effective and should not be used concurrently with glucocorticoids.
Contraindications
If the ear drum is ruptured or cannot be evaluated, proprietary ear drops are an ototoxicity risk.
Precautions
If the ear canal is swollen, ulcerated, and painful, cleaners and flushes containing acid, detergent, potent ceruminolytic agent, astringent, or alcohol should be avoided.
Interactions
Antibiotics, such as aminoglycosides (eg, gentamicin, neomycin) and fluoroquinolones (eg, enrofloxacin, marbofloxacin), are inactivated by acidic solutions.
To prevent transport of drugs into the inner ear, dimethyl sulfoxide (DMSO)-containing products should not be used in combination with aminoglycosides.
Follow-Up
Patient Monitoring
The patient should be checked 10–14 days after starting therapy.
The ear should be reexamined to assess improvement and patient status.
Cytology should be performed to gauge effectiveness of topical therapy.
Adjust therapy if response is inadequate.
Rechecks may be performed q2wk until the canal has healed and cytology results are negative for bacteria and inflammatory infiltrate.
Prevention
Owners should be taught effective ear cleansing techniques and how to recognize early signs of recurrence.
Suitable maintenance flushes include those containing acetic acid or tris-EDTA.
Identification and treatment of predisposing causes are necessary.
The patient should be reevaluated with otoscopic examination and cytology regularly (ie, every few months).
In General
Relative Cost
Flush solutions: $
Topical antibiotics (first line): $
Topical antibiotics (second line): $–$$
Topical antibiotics (off-label): $
Take-Home Points
Pseudomonas otitis can occur in cats and dogs of any age.
Predisposing factors for Pseudomonas otitis are those that disrupt normal ear canal environment and allow bacterial invasion.
All Pseudomonas otitis cases can benefit from thorough cleansing.
Systemic and topical glucocorticoids reduce exudate formation and swelling, cleansers and flushes remove debris and inflammatory mediators, and topical antibiotics are useful and widely available.
Owners should be taught effective cleansing techniques and how to recognize signs of recurrence.