Exploratory Laparotomy in the Dog & Cat
Exploratory laparotomy is routinely performed in small animal practice and is indicated when organ dysfunction or trauma involving the abdominal cavity requires definitive diagnosis along with surgical treatment and prognosis.1 Surgical exploration provides information through inspection, palpation, and/or hollow organ luminal mucosa observation. Samples can be obtained for microbiologic and cytologic examination or biopsy for histopathologic examination. Abdominal exploration should be performed in a timely manner to increase the likelihood of successful diagnosis and management without negatively affecting the patient.
A ventral midline laparotomy of adequate length from xiphoid to the pubis is the standard approach to explore the entire abdominal cavity in a systematic manner.
A ventral midline laparotomy of adequate length from xiphoid to the pubis is the standard approach to explore the entire abdominal cavity in a systematic manner. Every surgeon may develop his or her own technique, but a suggested method includes exploring the cranial quadrant (diaphragm; liver, gallbladder, and biliary tree; spleen and stomach; duodenum and pancreas), caudal quadrant (jejunum, ileum, and colon; urinary bladder; urethra and prostate or uterus), right paravertebral region by retracting the mesoduodenum, and left paravertebral region by retracting the mesocolon (kidneys, adrenal glands, ureters, and ovaries).2
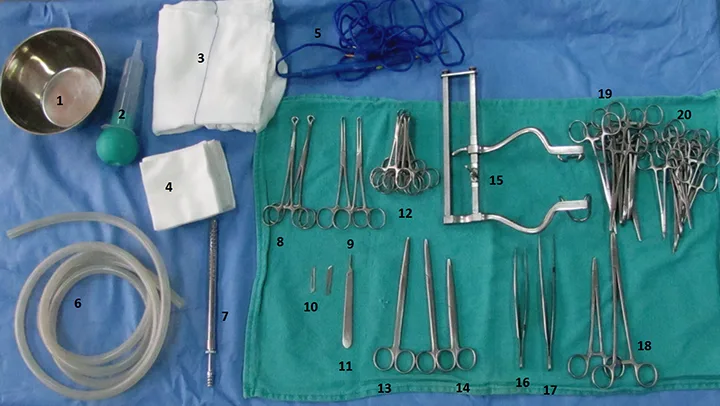
What You Will Need
Surgical bowl
Bulb syringe for irrigation
Laparotomy pads
4 x 4” (10.2 cm x 10.2 cm) gauze sponges
Monopolar diathermy cable
Suction tube
Poole suction tip
Babcock tissue forceps
Allis tissue forceps
No 15 and 10 scalpel blades
Bard Parker scalpel handle
Backhaus towel clamps
Curved and straight Metzenbaum scissors
Straight Mayo scissors
Balfour retractors
Debakey tissue forceps
Rat-tooth thumb forceps
Mayo-Hegar needle holders
Straight and curved Rochester-Carmalt hemostatic forceps
Straight and curved mosquito hemostatic forceps

Step 1.
Generously clip and prepare the surgical site, extending cranially to the xiphoid, caudally to the pubis, and over 5 to 10 cm from the ventral midline on either side. Express the bladder through the abdominal wall.
Author Insight:
Midline laparotomy incision should extend from xiphoid to pubis.