Episodes of Weakness & Hypoglycemia in a Dog
A 13-year-old spayed female German short-haired pointer was presented for episodes of hindlimb weakness during long walks.
History. The episodes had occurred over the past 2 months. The dog was otherwise healthy and had no pertinent medical history.
Physical Examination. The dog was bright, alert, and responsive. Abdominal palpation was nonpainful, and no masses or organomegaly was detected. She was ambulatory in all 4 limbs, and no lameness was noted. Cranial nerve testing and peripheral reflexes were within normal limits, and no weakness was observed.
Laboratory Results. In-house packed cell volume was 45% and total solids were 7.2 mg/dL. Blood glucose level on presentation was 56 mg/dL. Complete blood count and urinalysis were unremarkable. Chemistry panel revealed hypoglycemia (54 mg/dL; reference range, 60-120).
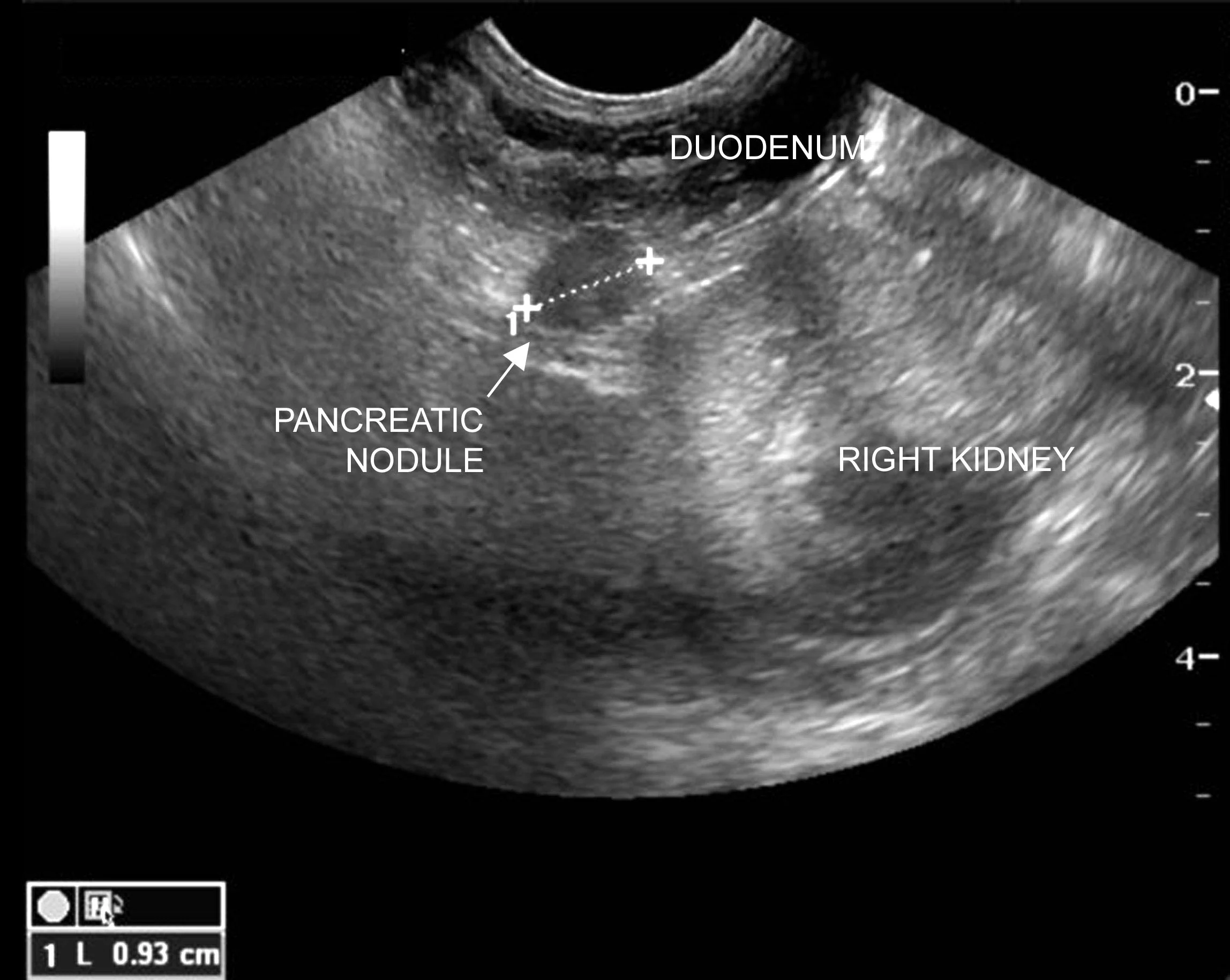
Diagnostic Imaging. Abdominal ultrasonography performed to examine the pancreas revealed a 1.4 × 0.93 × 0.87 cm hypoechoic mass in the right limb (Figure 1, arrow). No other abnormalities were found. Three-view thoracic radiographs to evaluate for presence of metastatic pulmonary disease (due to the diagnosis of the pancreatic tumor) were unremarkable (Figures 2 and 3).ASK YOURSELF...Which of the following diagnostic tests should be done next in this dog?A. Serum growth hormone levelB. Total thyroxineC. Glucose curveD. Insulin levelE. Urine culture and sensitivity
Correct Answer: DInsulin level
Discussion. Insulinoma is the most likely cause of hypoglycemia in a dog with a pancreatic mass. Insulinomas are functional tumors arising from the beta cells of the pancreatic islets. The cause of hypoglycemia in dogs with insulinomas is autonomous synthesis and release of insulin from the neoplastic beta cells despite hypoglycemia.1
Clinical signs, such as weakness, collapse, seizures, ataxia, muscle fasciculations, posterior weakness, depression, and lethargy, are commonly episodic because fasting, exercise, and possibly excitement can exacerbate hypoglycemia and trigger clinical signs.1 A random or fasting blood glucose level less than 60 mg/dL in non-toy breed, nonjuvenile dogs should always prompt further investigation.
Differential Diagnosis. Differential diagnoses for hypoglycemia in adult dogs include artifactual hypoglycemia, acquired hepatic dysfunction, Addison's disease, non-beta cell tumors (such as hepatocellular carcinoma and leiomyoma/leiomyosarcoma), sepsis, uremia, congenital hepatic disease, severe polycythemia, and iatrogenic hypoglycemia.1
Diagnosis. A diagnosis of insulinoma is made when the serum insulin level is high (> 10 µU/mL) in conjunction with hypoglycemia (< 60 mg/dL). In this patient, at the time of documented hypoglycemia (54 mg/dL), the insulin level was 38 µU/mL.
A mass in the pancreas is rarely detected by ultrasonography; thus, absence of a mass should not be cause for ruling out the presence of insulinoma.2 Ultrasonography is useful for screening for metastatic disease to such sites as the intraabdominal lymph nodes and liver.1 Computed tomography identifies most insulinomas; however, intraoperative inspection and palpation of the pancreas remain the best diagnostic tests.2
Treatment. If insulinoma is suspected, exploratory laparotomy should be performed. Complete excision of a focal tumor may be curative; however, this is rare because metastasis at time of diagnosis is common.1 If the tumor cannot be completely removed, debulking should be performed in an attempt to achieve remission or at least alleviation of clinical signs.1
If surgery is not an option or the tumor cannot be excised, medical therapy should be instituted. The goal is to control clinical signs, not to attain normal blood glucose. Dogs should be fed frequent, small meals. Glucocorticoids, such as prednisone, should be added when dietary changes alone are no longer effective. Other less common therapies include use of diazoxide, octreotide, and streptozotocin.
Diazoxide, a benzothiadiazide diuretic, inhibits insulin secretion, stimulates hepatic gluconeogenesis and glycogenolysis, and inhibits tissue use of glucose.1 Octreotide is a somatostatin analog that inhibits insulin synthesis and release.1 Streptozotocin is a nitrosourea that selectively destroys pancreatic beta cells.3 Use of diazoxide, octreotide, and streptozotocin is not routine, and the efficacy and safety of these drugs need further investigation.
Prognosis. Prognosis is generally guarded, although some dogs can be cured by surgery alone.1 Median survival time in dogs treated with surgical excision of the tumor is around 12 to 18 months compared with 2.5 months for medical management alone.4,5
Patient Follow-Up. In this patient, exploratory laparotomy revealed a mass in the right limb of the pancreas, which was resected. A pancreatic lymph node was mildly enlarged. Histopathology of the mass and lymph node was consistent with insulinoma. Chemotherapy with streptozotocin was recommended but declined by the client.
Following surgery, the patient was fed small, frequent meals, which maintained normoglycemia for 11 months; then, multifocal nodules in the liver were detected and suspected to be consistent with metastatic disease. Glucocorticoid therapy has controlled clinical signs for 3 months since that finding.
Tx at a glance• Surgical excision, or at least debulking, is the best choice for long-term control of blood glucose.• Feeding small, frequent meals of diets high in fat, complex carbohydrates, and fiber is recommended.• Glucocorticoid therapy (prednisone, 0.5 mg/kg/day divided twice daily) can be added if dietary changes do not control clinical signs.• More advanced medical therapies include diazoxide, octreotide, and the chemotherapeutic agent streptozotocin.
Take-Home Messages• Blood glucose < 60 mg/dL in a fasting or nonfasting adult dog should prompt further investigation.• Always remeasure blood glucose if hypoglycemia is documented once, as artifactual hypoglycemia is common.• Suspicion of an insulin-secreting tumor can be confirmed if a high insulin level is detected in conjunction with a low glucose level (< 60 mg/dL).• The best diagnostic test for insulinomas is surgical exploration of the abdomen with palpation of the pancreas.• Metastatic disease to lymph nodes in the abdomen or liver is common at the time of diagnosis of insulinomas.
EPISODES OF WEAKNESS & HYPOGLYCEMIA IN A DOG • Andrea B. Flory
References1. Beta-cell neoplasia: Insulinoma. Feldman EC, Nelson RW. In Canine and Feline Endocrinology and Reproduction, 3rd ed-St. Louis: Elsevier, 2004, pp 616-644.2. Comparison of ultrasonography, computed tomography, and single-photon emission computed tomography for the detection and localization of canine insulinoma. Robben JH, Pollak YW, Kirpensteijn J, et al. J Vet Intern Med 19:15-22, 2005.3. Streptozotocin for treatment of pancreatic islet cell tumors in dogs: 17 cases (1989-1999). Moore AS, Nelson RW, Henry CJ, et al. JAVMA 221:811-818, 2002.4. Outcome of surgical versus medical management of dogs with beta-cell neoplasia: 39 cases (1990-1997). Tobin RL, Nelson RW, Lucroy MD, et al. JAVMA 215:226-230, 1999.5. Improved survival in a retrospective cohort of 28 dogs with insulinoma. Polton GA, White RN, Brearly MJ, Eastwood JM. J Small Anim Pract 48:151-156, 2007.