Emergency Management of Urethral Obstruction in Male Cats
Catherine V. Sabino, DVM, DACVECC, Red Bank Veterinary Hospital, Tinton Falls, New Jersey
Ainsley Boudreau, DVM, DACVECC, Toronto Veterinary Emergency Hospital
Karol A. Mathews, DVM, DVSc (Surgery), DACVECC, University of Guelph

How can I best diagnose, stabilize, and treat feline patients with urethral obstruction?
Urethral obstruction in cats usually occurs in males between 2 and 10 years of age. It is far less common in female cats because of the wider, shorter formation of the urethra.
Causes of urethral obstruction include:
Anatomic or physical
Urethral plugs
Obstructive idiopathic urethritis
Urolithiasis (with or without bacterial infection)
Urethral stricture
Less frequently, neoplasia
Functional
Urethral spasm
Diagnosis & Assessment
Clinical Signs
The classic sign in cats with obstruction is vocalization and straining while posturing to urinate. Other, less specific, signs can vary from vomiting and mild lethargy to profound lethargy and weakness or collapse.
Physical Examination
Diagnosis is based on the presence of a nonexpressible urinary bladder, which is usually large and firm on palpation. It should be noted, however, that patients who have been obstructed for a shorter period of time may have smaller urinary bladders at the time of physical examination. Care should be taken to gently palpate the urinary bladder because mucosal injury from distention can weaken the bladder wall and make it susceptible to leakage and tearing. A partially obstructed bladder may be managed with analgesia and antispasmodic therapy and the patient can be evaluated for ability to urinate. However, if the bladder remains nonexpressible, catheterization may be required.
Initial Diagnostics
Minimum database: Blood for baseline electrolytes should be collected to evaluate for life-threatening electrolyte derangements.
If possible, baseline complete blood count and serum biochemical profile (for evaluation of renal parameters) can also be collected and performed at this time.
Additional Diagnostics
Other patient-dependent diagnostic testing may be done after urethral catheterization and fluid therapy have been initiated. These may include:
Urine sediment examination
Urinalysis
Urine culture
Abdominal radiography
Abdominal ultrasonography.
Urinary sediment may reveal pyuria (urinary tract infection), crystalluria, hemorrhage (cystitis), or abnormal cells (neoplasia). Crystal identification is recommended to guide future treatment and prevention.Samples should be collected during urethral catheter placement. If possible, a urine sediment examination should be prepared for slide evaluation within 30 minutes to prevent development of artefactual crystalluria.
Stabilization & Monitoring
Stabilization
All cats that present with urethral obstruction should be treated as an emergency. Analgesia and a short period of general anesthesia or heavy sedation (depending on patient stability) are necessary for the process of relieving the obstruction. It is important that cardiovascular stability is ensured as soon as possible and, if required, that the patient is prepared for general anesthesia.
Fluid administration depends on the individual patient.
For shock or poor perfusion, administer 5-mL/kg boluses of a buffered electrolyte solution until the patient improves: Boluses of a buffered balance electrolyte solution (eg, lactated Ringer solution) Ringer solution are recommended.
Otherwise, assess hydration (5% dehydration if signs are mild, 8% if moderate, and 12% if severe) and calculate fluid requirement. The maintenance fluid rate is in addition to this:
Percentage dehydration body weight (kg) = L
For example, the formula for 5% dehydration in a 3-kg cat would be: 5/100 3 = 0.15 L = 150 mL
Biochemical & Electrolyte Abnormalities
Many biochemical and electrolyte abnormalities occur in cats with urethral obstruction.
Hyperkalemia
Clinical signs of hyperkalemia are generally nonspecific, such as muscle weakness and profound lethargy. Bradyarrhythmias can indicate hyperkalemia, but there is no threshold potassium level that can predict the development of an arrhythmia. Monitoring the electrocardiogram (ECG) is the quickest way to document that a life-threatening hyperkalemia may affect myocardial function (Figure 1). Wide-complex tachycardia, as well as ventricular tachycardia, may also be present. ECG abnormalities will resolve with appropriate treatment of hyperkalemia.
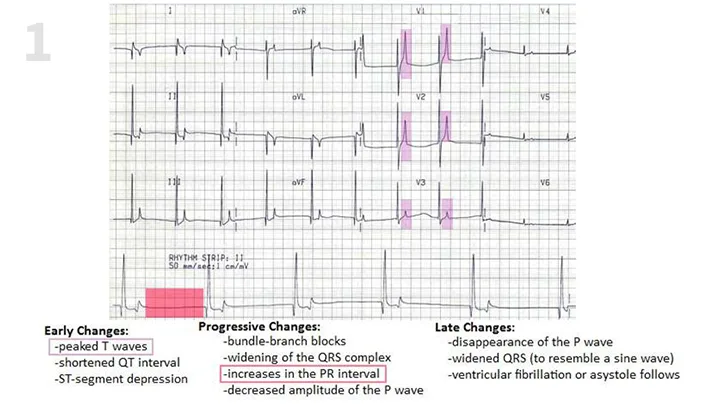
FIGURE 1 ECG changes seen with urethral obstruction. Image adapted with permission from Drs. Michael O’Grady and Lynne O’Sullivan; Veterinary Cardiology Online (vetgo.com)
ECG abnormalities and potassium levels 8 mEq/L(emergent treatment):
Administer 10% calcium gluconate (0.5 mL/kg IV over 510 min) while continuously evaluating ECG to allow stabilization of the heart until definitive treatment (see below) takes effect.
Calcium gluconate will not reduce potassium levels.
Arrhythmias due to hyperkalemia (definitive treatment):
Regular IV insulin (0.250.5 IU/kg) followed by an IV bolus of 50% dextrose (0.5 mL/kg, diluted 1:4 in 0.9% sodium chloride) and a continuous rate infusion of dextrose (2.5%5%) in a buffered balanced electrolyte solution. Insulin is preferred, if available, because it causes a faster decrease in serum potassium than dextrose alone.
If regular insulin is not available or potassium level is 6.5 to <8 mEq/L, 50% dextrose (0.5 mL/kg, diluted 1:4 in 0.9% sodium chloride) alone can stimulate release of endogenous insulin to drive potassium intracellularly and may be adequate for mild-to-moderate hyperkalemia when no other alternatives exist.
Mild hyperkalemia (potassium level <6.5 mEq/L):
Will resolve with IV volume expansion with a buffered balanced electrolyte solution.
Refractory hyperkalemia:
Can be seen in patients that have developed acute kidney injury secondary to urethral obstruction. If available, dialysis (peritoneal or hemodialysis) can be considered, particularly if hyperkalemia persists once the obstruction has been relieved.
Hypocalcemia
If hypocalcemia is documented, supplementation with 10% calcium gluconate (0.5 mL/kg IV) may need to be given over 5 to 10 minutes, with evaluation of a continuous ECG.
Acidosis
Most cases of metabolic acidosis can be corrected with IV administration of buffered balanced electrolyte solution fluid. Severe metabolic acidosis (total CO2or HCO3-level <10 mmol/L, or pH 7) may necessitate administration of sodium bicarbonate if not resolved with fluid therapy.
Treat acidosis if it is associated with bradyarrhythmia or an HCO3-level <12 mmol/L after appropriate fluid resuscitation (acidosis usually corrects after administration of alkalinizing fluids, improved perfusion, and establishment of diuresis):
Calculate bicarbonate requirement according to the following formula: (Normal HCO3- [ie, 20]) (Actual HCO3-) 0.3 body weight (kg)
Give half of this (diluted, can be administered via syringe pump, diluted into IV fluids in burette, or by slow IV push) over 30 minutes and monitor the ECG.
The hope is that treating acidosis will also treat hyperkalemia. If metabolic acidosis is not improved after bolus fluid therapy, continue with sodium bicarbonate The aim is not to correct to normal but to bring pH out of the critical zone (<7.2 or HCO3- <12 mmol/L).
Azotemia
Patients with urethral obstruction may have postrenal azotemia. Patients with prolonged urethral obstruction may also be severely dehydrated and have significant prerenal azotemia in addition to renal and postrenal azotemia. This is usually corrected with relief of the obstruction and IV administration of a balanced electrolyte solution.
Monitoring
When an arrhythmia has been documented, the patient should be closely monitored with continuous electrocardiography and indirect blood pressure measurement at frequent, regular intervals.
Patients with initial electrolyte abnormalities should have electrolytes reassessed 30 to 60 minutes after treatment to correct hyperkalemia; depending on the patients condition, reassessment should be repeated at variable intervals.
Physical examination and urine output monitoring should also be performed.
Treatment
Relief of Urethral Obstruction
Induce anesthesia with short-acting agents (Table). Ensure adequate sedation and analgesia to reduce the risk of movement or struggling during catheterization and to improve chance of successful catheterization. Severely debilitated patients may require only minimal sedation (such as a low dose of a short-acting opioid).
Sacrococcygeal epidural under sedation can be used for placement of a urinary catheter in cats. This technique may alleviate the need for further anesthesia or sedation to relieve an obstruction. This can be considered in patients for which alternative anesthesia is not possible because of unavailability of medications or contraindications to general anesthesia. Lidocaine, preferred for its rapid onset, can result in anesthesia after injection and last up to 60 minutes.
Attempt to induce voiding with gentle bladder palpation to confirm urethral obstruction. Patients with functional obstruction (eg, urethral dyssynergia or urethritis) may pass urine with gentle palpation of the bladder.
Apply sterile lidocaine gel (or 0.25 mL of sterile 2% lidocaine) in the urethral orifice. In addition, lubricate the catheter with sterile gel (with or without lidocaine) to aid in placement. Some lidocaine in the gel will be absorbed systemically through the urethral mucosa; however, a period of local analgesia is of beneficial.
Toxic dose of lidocaine is 2 mg/kg in cats; consider prior use of topical lidocaine.
Perform extrusion of the penis and examine the distal urethra. A small plug or calculus may be removed at this time by using gentle massage. To extrude the penis, use one hand to stabilize and retract the prepuce and the other to pass the catheter. Always start with the least rigid type of catheter available (Figure 2). If there is an assistant, the second person can retract the prepuce with one hand and stabilize the tip of the penis with the other hand; this leaves the other person with 2 hands to pass the catheter. Once the catheter has been advanced a few millimeters, the assistant can straighten the urethra as much as possible by releasing the hold on the penis and allowing for easier passage of the catheter.
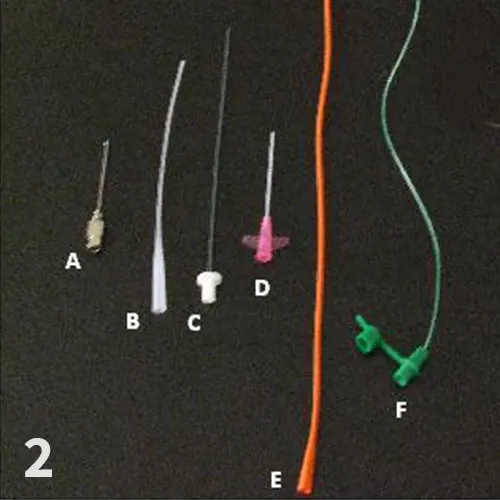
FIGURE 2 Types of catheters used to relieve urethral obstruction; all catheters are 3.5 to 5 Fr and arranged from most rigid (left) to least rigid (right): (A) olive-tipped catheter (21 gauge, 1.5 inch; jorvet.com); (B) tomcat catheter (3.5 Fr; sherwoodindustriesinc.com); (C) Slippery Sam Tomcat urethral catheter (3.5 Fr, 1.4 cm; smiths-medical.com); (D) BD Insyte-W IV catheter with stylet removed (20 gauge, 1.5 inch; bd.com/infusion); (E) red rubber catheter (3.55 Fr; sherwoodindustriesinc.com); (F) argyle feeding tube (3.55 Fr; tycohealthcare.co.uk).
If obstruction is not immediately relieved by catheter passage, try urohydropulsion using an open-ended tomcat catheter. Fill a 12-mL syringe with sterile saline and add a small amount of sterile lubricant jelly to the saline (shake into an emulsion) to lubricate the urethra during hydropulsion. A smaller syringe (ie, 3 mL) can be used for added pressure if initial attempts at hydropulsion are unsuccessful. Hold the prepuce, extend the penis dorso-caudally (make as straight a urethra as possible), and flush the penile urethra while advancing the catheter. Per rectal compression of the urethra with concurrent hydropulsion may help relieve the obstruction.
If obstruction cannot be resolved, the patient may require cystocentesis to decompress an overly distended bladder (very high back-pressure). Place a 22-gauge butterfly catheter, or a needle with extension and a 3-way stopcock, in the midpoint of the bladder to allow for a single penetration through the bladder wall. Remove as much urine as possible and submit the urine for urinalysis and urine culture. At this time, another attempt at urethral catheterization can be performed and is frequently successful with reduced back-pressure in the bladder.
Following placement of the urinary catheter, imaging should be used to confirm correct catheter placement prior to suturing it into place and to evaluate for the presence of uroliths. Abdominal radiographs (minimally, a lateral radiograph) or ultrasonographic examination can be performed. If straightforward diagnosis of obstructive uropathy is not apparent on radiographs, ultrasonographic or contrast urography is required. Evaluation of the upper and lower urinary tract may be required in selected patients.
Table 1: Emergency Care: Suggested Analgesic & Anesthetic Protocols for Cats
Stable patients: Normal mentation, well-hydrated, normal vital measures
Obtunded patients: Mild dehydration, mild depression, normal vital parameters
Nonstable patients: Patients with electrolyte abnormalities requiring stabilization prior to anesthesia
Other adjunctive method of analgesia:
Epidural anesthesia: Appropriate for all patients without a contraindication to epidural anesthesia; should be performed by clinicians with experience. DOSE: 0.1-0.2 mL/kg 2% preservative-free lidocaine. Patient should be sedated prior to epidural anesthesia being attempted. If effective (should be effective within minutes), the tail and rectum should relax and there should not be response to pinching of the tail. This will provide analgesia for up to 1 hour, so further analgesia will need to be considered on an ongoing basis.
Nonsteroidal anti-inflammatory drugs (NSAIDs): Appropriate only in patients without a contraindication for NSAID administration. Can be useful in cases where other analgesic options are unavailable or contraindicated. These medications should be dosed on ideal body weight to decrease the risk of adverse effects.
* Not all drugs are available in all markets, particularly opioids. For more information on this topic, visit WSAVA Global Pain Council.
Inpatient/Outpatient Care
Patients that are stable on presentation may not require hospitalization or an indwelling catheter once the inciting cause (eg, urethral plug) has been removed. These patients can be managed on an outpatient basis. However, for patients with metabolic abnormalities or a difficult obstruction, a urinary catheter should remain in place for 24 to 48 hours, or until the urine appears normal. These patients may be discharged from the hospital when normal, consistent voiding behavior is witnessed. If the cat cannot urinate, consider re-obstruction, bladder atony, urethral damage, urethral spasm, or reflex dyssynergia due to inflammation.
Alternative Treatments
Not all obstructions can be relieved via urethral catheterization. In these cases, patients can be stabilized and the bladder emptied by intermittent cystocentesis or placement of a cystostomy tube while awaiting definitive diagnosis and treatment. The latter should be performed as soon as possible to avoid complications associated with intermittent cystocentesis.
Continuing Medical Therapy
Opioids (eg, buprenorphine, hydromorphone, methadone, fentanyl) at lowest dose needed to attain comfort can be used for analgesia and to help relax the urethral sphincter.
Use of anti-inflammatory therapy may reduce inflammation and discomfort in cats straining because of inflammation. In the authors experience, this can be beneficial in reducing inflammation and dyssynergia postobstruction.
Nonsteroidal anti-inflammatories:
Meloxicam (initial dose: 0.050.1 mg/kg IV, SC, or PO once a day)
Robenacoxib (initial dose: 2 mg/kg SQ once a day, 6mg per CAT 2.5-6kg; 12 mg per CAT 6.1-12 kg PO once a day)
NOTE: For use in stable patients with normal hydration levels only. Labelled dosing schedule (length, dose and frequency) may vary by country.
All NSAID medications should be dosed on ideal body weight to decrease the risk of adverse effects.
Corticosteroids:
Dexamethasone (0.06 mg/kg 0.16 mg/kg IV or IM once a day)
Prednisolone (0.5-1 mg/kg PO once a day dose can be divided)
Alpha-1 adrenergic antagonists can be used to decrease urethral tone.
Phenoxybenzamine (2.5-7.5 mg once to twice a day)
Prazosin (0.5 mg 3 times a day)
Acepromazine (0.01-0.05 mg/kg IV) can also be used to promote relaxation of the urethral sphincter.
Parasympathomimetics (ie, bethanechol) should be used only in animals that have bladder atony secondary to severe prolonged distention of the bladder, and only once urethral patency is confirmed and there is no evidence of remaining calculi.
Follow-Up
After successful medical management, owner counseling about long-term management of the underlying cause is necessary. Internal medicine textbooks (eg, Small Animal Internal Medicine) can be used to obtain information about treatment of urinary tract infections, crystalluria, and urolithiasis. If medical management fails repeatedly or all medical options have been exhausted, surgical treatment (perineal urethrostomy) may be indicated.
Complications
Torn Urethra
During placement of a urinary catheter, the urethra can be torn, especially if the patient is moving. This is determined by feeling a pop through a band of tissue and an absence of urine flow into the catheter. It can be confirmed radiographically (visualization of the urinary catheter outside of the urethra) or via contrast cystography. Treatment involves leaving an indwelling urinary catheter in place for 72 hours to 7 days and allowing the tear to heal by second intention. Healing can be evaluated by clinical signs or can be confirmed via contrast cystography. To decrease risk for urethral damage, the softest catheter possible should be used; more rigid types should only be used if passing the soft catheter is unsuccessful (Figure 2).
Uroperitoneum
Uroperitoneum can result from bladder rupture, either iatrogenic or noniatrogenic. Treatment may involve exploratory laparotomy and surgical correction if conservative management (ie, urinary catheterization and abdominal drain placement to allow continuous evacuation and lavage) does not allow healing of tissues. Small defects in the urinary bladder, such as those caused by cystocentesis, may heal with conservative management. In cases of septic peritonitis secondary to leakage of infected urine, surgical management should be performed. An abdominal drain (Jackson-Pratt drain or closed-system catheter placed by sterile Seldinger technique) can be placed, in addition to placement of a urethral catheter, before definitive surgical correction is performed.
Diuresis & Azotemia
Post-obstructive diuresis frequently occurs with prolonged obstruction. High rates of IV balanced electrolyte solution are initially required to compensate for losses; therefore, careful balancing of the patients ins (fluid administration) and outs (quantification of urine production) is necessary. BUN or creatinine level (BUN stick may also be adequate) should be monitored daily, and fluid therapy can be tapered after azotemia resolves. Urine production can be measured via a closed urinary catheter-collection system and calculated as mL/kg per hour and compared with normal urinary production during receipt of IV fluids (1-2 mL/kg per hour). If definitive urine output is unknown (eg, catheter malfunction or removal), changes in hydration status and body weight can be used as a more crude assessment of fluid balance. (Weigh the cat 2-4 times daily; a change in body weight of 0.1 kg is equal to a fluid loss or gain of 100 mL). If a urinary catheter cannot be maintained, urine can be collected by using nonabsorbing cat litter and then measured.