Diagnosis & Management of Otitis
Profile
Definition
Otitis is inflammation of the ear structures. It is not an infection.
Systems
The external ear canal epidermis, eardrum, and middle ear are affected by otitis. Dogs acquire otitis media from erosion and perforation of the eardrum with extension into the bulla. In cats with chronic upper respiratory infection, the middle ear may become affected by extension via the eustachian tubes. The hair cells in the cochlea and semicircular canals may be damaged by chemicals or infected with bacteria. Trauma to nerves in and around the ear often causes neurologic signs. Bone and cartilage can be affected by infection and inflammation.
Incidence/Prevalence
Twenty percent of all dogs in the United States have otitis externa; incidence is higher in warm, humid regions. The incidence is higher in breeds with genetic predisposition to allergic disease and in those breeds with increased cerumen glandular density. About 7% of cats have otitis externa; ear mite infestations and otitis media are also found in cats.
Signalment
Species
Otitis externa and otitis media can occur in both dogs and cats.
Breed Predilection
Many breeds of dog have a genetic predisposition to allergy. Golden retrievers and Labrador retrievers are overrepresented (perhaps due to their popularity); however, many other breeds, such as cocker spaniels, springer spaniels, and poodles, have a high incidence of otitis externa. Noninfectious primary secretory otitis media, or "glue ear," in Cavalier King Charles spaniels causes a painful buildup of mucus in the bulla and a bulging or ruptured eardrum. This may result from a functional drainage problem in the auditory tube. There does not seem to be a breed predilection in cats.
Age and Range
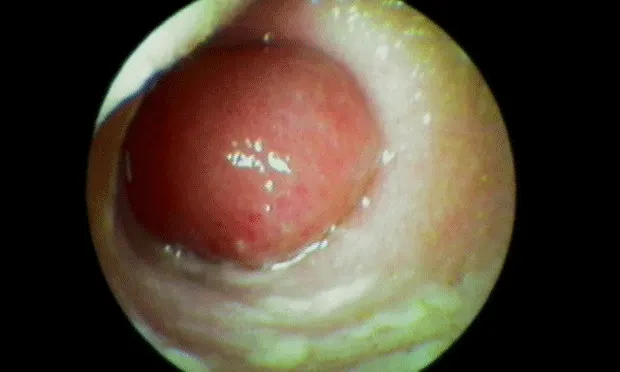
Otitis externa can occur in very young puppies and kittens due to ear mites. Puppies can also manifest adverse food reactions early in life, resulting in ear canal inflammation. Young adult cats with middle ear disease may present with nasopharyngeal polyps (Figure 1). Middle-aged dogs with atopic dermatitis seem to represent the largest portion of dogs with otitis. Older dogs with otitis may have chronic ear problems.
Figure 1. Inflammatory polyp in the horizontal ear canal of a cat.
Causes
The primary causes of otitis externa are atopic dermatitis, adverse food reactions, ear mites, and in some cases hypothyroidism. Other causes include trauma from instruments or cotton swabs. In cats, a significant cause of ear disease is chronic upper respiratory infections and subsequent otitis media.
Risk Factors
Risk factors include those that affect ventilation of the ear canal-humidity, oxygen tension, composition of the cerumen, temperature, and conformation of the ear canal and pinna. Failure to detect and treat ear disease early can lead to significant changes to the ear canal. Stenosis, tumors, excessive hair, excessive wax, hyperplastic glands or epithelium, and ulceration exacerbate the disease.
Pathophysiology
Otitis Externa
In dogs, inflammation results from a skin disease that causes swelling of the ear canal. Closure of the lumen increases humidity and temperature while decreasing ventilation and decreasing oxygen level. The epithelial surface changes, exposing surface receptors, which then attach to bacteria and yeasts and result in infection. Increased blood supply to the ceruminous glands and sebaceous glands changes the amount and composition of the triglycerides and free fatty acids in the cerumen, turning them into substrates for bacteria and yeasts. Volatile fatty acids are produced, which perpetuate inflammation.
Otitis externa is rare in cats and usually results from traumatic damage from ear mites.
Otitis Media
In dogs, secondary otitis media is caused by otitis externa extending through the eardrum. Bacteria, yeast, hairs, cells, enzymes, and medications pass through the eardrum into the bulla of the middle ear. The foreign matter incites inflammation and increases secretion of mucus from the mucous membrane.
In cats, primary otitis media results when organisms from the retropharynx ascend through the auditory tube into the tympanic bulla. Inflammation, polyps, and infection in the bulla result in copious mucus and pus formation. Pressure from these secretions causes pain and pressure on the eardrum, resulting in rupture.
Signs
Dogs and cats with otitis externa or otitis media have pain and pruritus. Signs of otitis include scratching, head shaking, rubbing the ears, redness, odor, otic discharges, and sometimes aural hematoma. The pinna may become hyperplastic or indurated. With deeper ear problems, neurologic signs, such as head tilt and/or nystagmus, vestibular disease, Horner's syndrome, facial nerve palsy, and deafness, may occur.
History
In addition to the signs noted above, in a dog with erect ears, the ears may flop down from otic pain. With otitis media and otitis interna, neurologic signs may be present. Unilateral keratoconjunctivitis sicca may also result from facial nerve damage.
Physical Examination
Pain on manipulation of the pinna indicates an ear problem. Ossification of the ear canals indicates a serious, long-standing problem. Small cerumen gland adenomas and waxy accumulations may be present on the concave pinna. Odors or abnormal discharge causing wetness of the concave pinna may be detected. The pinna is usually reddened because of scratching or inflammation. In dogs with otitis externa, otoscopic examination of the ear canal may reveal exudate, erythema, glandular hyperplasia, epithelial hyperplasia, ulceration, or wax accumulation.
If hairs are absent, there are enzymes present. Ear mites, chiggers, ticks, foreign bodies (including plant material), insects or insect parts, or other material can be seen on otoscopic examination. With ear canals that are occluded from edema, a short course of steroid therapy may be needed to open the canals before otic examination.
Pain Index
The density of nerve endings increases with the depth of the ear canal. Pinnal diseases are more pruritic and less painful than vertical ear canal disease. Horizontal canal disease and middle ear diseases are very painful and often require adjunctive pain medication.
Diagnosis
Definitive Diagnosis
On otoscopic examination, the epidermis of the ear canal is erythematous, thickened, and roughened and usually has an exudate. Gram stains can be done, but they do not usually add much information. Epithelium can be macerated, eroded, or exfoliated (Figure 2).
Figure 2. Severely inflamed, swollen, macerated ear canal in a German shepherd
Differential Diagnosis
Many conditions cause pruritus around the ear canal and can be mistaken for otitis externa.These include sarcoptic mange, juvenile cellulitis, fleas, and foreign bodies in the ear canal.
Laboratory Findings/Imaging
Cytology of otic exudates using mineral oil and/or Wright's-Giemsa stain reveals mites (both Demodex and Otodectes), bacteria, yeast, neutrophils, and other cellular debris.
Culture and sensitivity are commonly done but do not give accurate information and should be reserved for nonresponsive bacterial infections or purulent otitis media. When bacterial culture is performed, results should always be evaluated in conjunction with cytologic examination of exudate.
Imaging of the ear canals and tympanic bullae is best done using an open-mouth view with the nose pointed up at the head of the radiograph unit. Computed tomography and magnetic resonance imaging can also be used to determine the extent of stenotic ear disease or otitis media. Treatment Inpatient or Outpatient Otitis externa is usually treated on an outpatient basis; however, painful or fractious animals may occasionally require sedation and hospitalization. Otitis media cases require short-term anesthesia to flush the bulla, so hospitalization may be required. Medical Otitis externa is treated using eardrops with various medications. Otitis media is treated by medical or surgical means.
Treatment
Inpatient or Outpatient
Otitis externa is usually treated on an outpatient basis; however, painful or fractious animals may occasionally require sedation and hospitalization. Otitis media cases required short-term anesthesia to flush the bulla, so hospitalization may be required.
Medical
Otitis externa is treated using eardrops with various medications. Otitis media is treated by medical or surgical means.
Surgical
Proliferative and chronic external ear disease may be treated using either lateral ear canal resection (Lacroix-Zepp procedure) or vertical ear canal ablation. Lateral ear canal resection may leave too much proliferative, infected tissue in situ to benefit the patient.
Otitis media is a surgical disease, with either myringotomy or bulla osteotomy often required to remove exudate and infected soft tissue before resolution can be achieved. I sometimes use total ear canal ablation and lateral bulla osteotomy in cases of unresponsive otitis media/externa. Cats with nasopharyngeal polyps may require ventral bulla osteotomy or endoscopic traction-avulsion of the polyp mass.
Medications
Drugs & Treatment Options
Systemic corticosteroids reduce swelling in the ear canal and relieve the pain associated with inflammation. Many otic products also contain powerful topical corticosteroids. Less potent hydrocortisone products are available for maintenance.
Ear cleaners and ear flushes disinfect and dry the ear canals. Some ear cleaners contain detergents to remove waxes, alcohols to dry the ear canal, and acids to retard the growth of yeasts; others contain disinfectants. Newer ear flushes contain tris-EDTA, which helps to kill gram-negative organisms, such as Pseudomonas.
Topical antibiotics such as neomycin, gentamicin, and enrofloxacin are available in commercial products for bacterial infections of the ear canal. Other antipseudomonal drugs, such as tobramycin, ticarcillin, ceftazidime, and amikacin may be compounded. Some systemic intracellular antibiotics, such as fluoroquinolones, clindamycin, and azithromycin, may be helpful in the external and middle ear and target inflammatory sites.
Antifungal topical medications, aimed at Malassezia yeasts, include clotrimazole, miconazole, ketoconazole, nystatin, and thiabendazole.
Ear wicks are used in stenotic ears that are difficult for the owners to treat (Figure 3). The compressed sponge is inserted into the ear canal, moistened with aqueous steroid ear medication, and kept in place for 2 weeks. The sponge swells and conforms to the ear canal, keeping medication in constant contact with the ear canal epithelium.
Figure 3. Compressed ear wick before moistening (A). The ear wick expands up to a 9-mm diameter when wet (B).
Pain Management
Opioids, such as buprenorphine, butorphanol, and tramadol, help relieve ear pain. Some nonsteroidal antiinflammatory drugs may also help to reduce pain; however, NSAIDs should not be combined with systemic glucocorticoids, which are frequently used for ear disease.
Contraindications
Ototoxic agents (ie, gentamicin, polymyxin, and chlorhexidine products) should be avoided if the eardrum is compromised or cannot be evaluated.
Precautions
Acids, detergents, and alcohols should not be used in ulcerated ears.
Interactions
Ensuring that medications are compatible is essential. Aluminum acetate (Burow's solution) will precipitate enrofloxacin. Dexamethasone injection with propylene glycol will precipitate many antibiotics. Dexamethasone sodium phosphate solution should be used in compounding solutions. Acid ear cleaners can nullify the effect of some antibiotics, such as gentamicin. Dimethyl sulfoxide (DMSO) products should be avoided when using aminoglycosides to prevent transport of the drug through ear tissues into the inner ear.
Follow-Up
Patient Monitoring
The patient should be rechecked 2 weeks after initiation of topical therapy. This includes otoscopy to compare pretreatment pathology to current status and cytology to determine effectiveness of topical therapy. Changes in medication may be required if organisms remain. Occasionally, the original organism is gone (ie, Pseudomonas), but another organism that requires different treatment is present (ie, Malassezia).
Prevention
Home measures should include preventing the ears from getting wet during bathing or swimming. In addition, proper client education about use of prescribed medications or ear cleaners will help prevent errors. For example, in unilateral ear disease, the client needs to know which ear is affected to prevent the wrong ear from being treated. I like to shave the hair around the affected ear as a reminder.
TX at a Glance
Based on Otoscopic, Cytologic, & Microbiological EvidenceAlways clean wax and debris out of the ears before beginning any topical treatment. If ears are stenotic, this process may be delayed until after a short course of glucocorticoid treatment. Patients with painful ears should be anesthetized for deep ear cleaning.
Medical
Inflammation
Systemic
Dexamethasone injection (2 mg/ml): 0.2 mg/kg once every 2 weeks $
Prednisone: 1-2 mg/kg divided Q 12 H, reduce after 2 weeks. $ Topical • Fluocinolone/dimethyl sulfoxide (Synotic, www.fortdodge.com) $
Topical
Fluocinolone/dimethyl sulfoxide (Synotic, www.fortdodge.com) $
Topical dexamethasone sodium phosphate 1% ophthalmic solution $
Betamethasone $
Triamcinolone $
Mometason $
Bacteria
Topical
Gentamicin (Otomax & Mometamax, www.schering-plough.com) $
Enrofloxacin (Baytril Otic, www.bayer-ah.com) $
Neomycin (Panalog, www.fortdodge.com; Tresaderm, www.merck.com) $
Tobramycin 0.3% & dexamethasone (TobraDex ophthalmic, www.alcon.com); or 2 - 5 ml generic tobramycin 0.3% ophthalmic bottles and 1 ml dexamethasone SP $
Compounded generic ceftazidime ear drops: To a 2-g vial of ceftazidime, add 10.5 ml sterile water. Divide the 12 ml of solution into three 4-ml aliquots. Add 10 ml of sterile water to 1 of the aliquots and freeze the others. In 1 week defrost 1 frozen 4-ml aliquot, add 10 ml of sterile water and make another fresh bottle. $
Note: Oil-based medications are not recommended in purulent otitis.
Injectable
Compounded enrofloxacin (Baytril injection, www.bayer-ah.com) with dimethyl sulfoxide/fluocinolone (Synotic, www.fortdodge.com) ear drops. Mix 1 ml Baytril in 8 ml
Synotic. Discard after 1 week. $
Enrofloxacin in tris-EDTA at 10 mg/ml $
Yeast
Acetic acid/boric acid (Malacetic, www.dermapet.com) daily for 10 to 14 days; then weekly for maintenance $
Miconazole 1% solution Q 12 H for a minimum of 2 weeks. May add 1 ml dexamethasone SP per 30-ml bottle. $
Clotrimazole 1% solution (found in many topical combination ear products) Q 12 H for a minimum of 2 weeks $
Ketoconazole 1% (found in T8 Keto Flush [www.ivxanimalhealth.com] and Triz Ultra Plus Keto [www.dermapet.com]). Use daily for a minimum of 2 weeks to prevent yeast growth after bacterial infection. $
Surgical
Intraotic laser surgery $$$
Lateral ear canal resection $$$
Vertical ear canal resection $$$
Ventral bulla osteotomy (lateral bulla osteotomy for cats) $$$$
Total ear canal ablation and lateral bulla osteotomy $$$$$
EDTA = ethylenediaminetetraacetic acid