Detection & Treatment of Pneumothorax
Anthony Johnson, DVM, DACVECC, Veterinary Information Network
Pneumothorax, the accumulation of free air in the thoracic cavity, specifically between the lung and the thoracic wall, is most often a result of blunt trauma (eg, vehicular trauma). However, it may also occur spontaneously or secondary to penetrating thoracic injury, bullae rupture, or diseases such as severe pneumonia or neoplasia.
Dyspnea, open-mouthed breathing, cyanosis, tachypnea, and/or dull lung fields on auscultation should alert clinicians to the possibility of pneumothorax and prompt consideration of thoracentesis. If clinically indicated, thoracentesis should be performed before thoracic radiographs are taken, as trauma patients often cannot withstand the rigors of radiography without clinical stabilization. On the other hand, clinically silent pneumothorax does not always warrant thoracentesis, but these patients do require close observation and monitoring of respiratory effort.


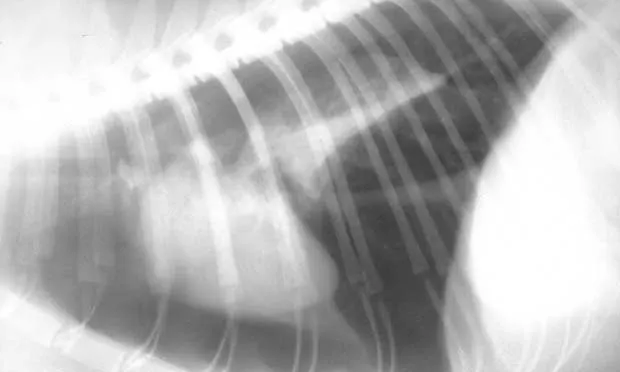
Pneumothorax is evident in this thoracic radiograph of a cat (A), as the cardiac silhouette is elevated from the sternum on the lateral projection and the lung lobes are collapsed. Close-up of the lateral view (B) shows air between the sternum and cardiac silhouette. In my experience, the lateral view is more sensitive for detecting pneumothorax because the elevation of the heart from the sternum is easily appreciated. When viewed from dorsoventral (DV) or ventrodorsal (VD) positioning, the lack of blood vessels extending out to the periphery and increased lucency of the lung fields could be overlooked.
If indicated, thoracentesis should be performed bilaterally above the level of the costochondral junction, between the 6th and 10th intercostal spaces. The intercostal vessels and nerves (known as the neurovascular bundle) are located caudal to the ribs. The needle should be introduced cranial to the rib if possible. In some patients (eg, obese patients or those with significant chest wall pathology), accurately identifying the rib margins may be difficult.


Signs of retraction of the lung lobes from the thoracic wall and blunting of the costophrenic angles (A) are best appreciated on the DV view (versus VD view) unless a large amount of air is present. Close-up of the DV view (B) shows air between the thoracic wall (white arrows) and lung (black arrows).
Some patients with pneumothorax can be clinically managed with a single thoracentesis, whereas other patients require placement of a thoracostomy tube. In general, if thoracentesis is performed more than 3 times in a 24-hour period, use of a chest tube may be indicated. Chest tube placement, however, may not be required if the volume of removed air decreases with each successive tap.
DV = dorsoventral, VD = ventrodorsal
For more information see Acute Respiratory Distress: The Blue Patient by Drs. Stacey Leach & Deborah Fine in the February 2011 issue of Clinician’s Brief.
Also read the following articles:
Pneumothorax—Identified with Minimal Training?Acute Respiratory Distress: The Blue PatientInterpreting Small Animal Thoracic Radiographs
Images courtesy of William Blevins, DVM, MS, Diplomate ACVR